INDICATIONS: SUPERIOR OBLIQUE MUSCLE PALSY
The superior oblique muscle may need to be strengthened to correct vertical strabismus in the setting of a clinically underacting muscle. The main indication for superior oblique strengthening is congenital or acquired superior oblique muscle palsy. Less frequently, strengthening may be helpful to treat residual inferior oblique muscle overaction and V-pattern after inferior oblique muscle weakening in patients with persistent underaction of one or both superior oblique muscles.
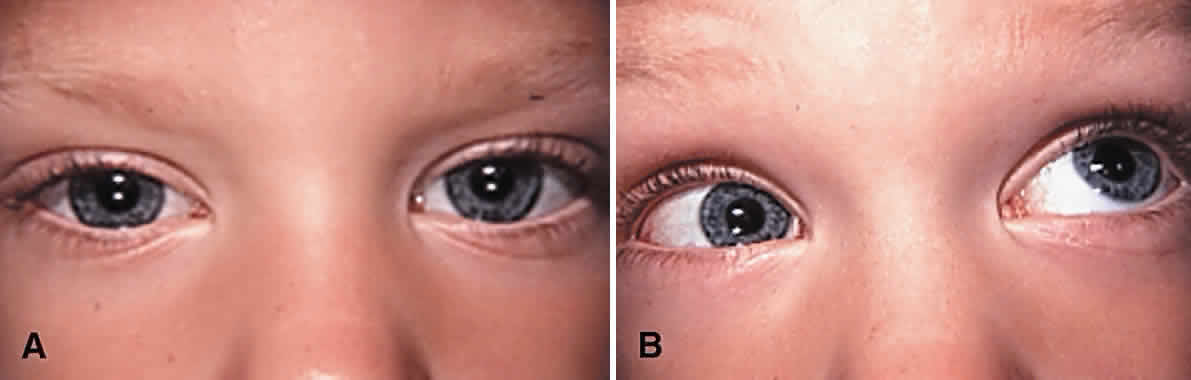
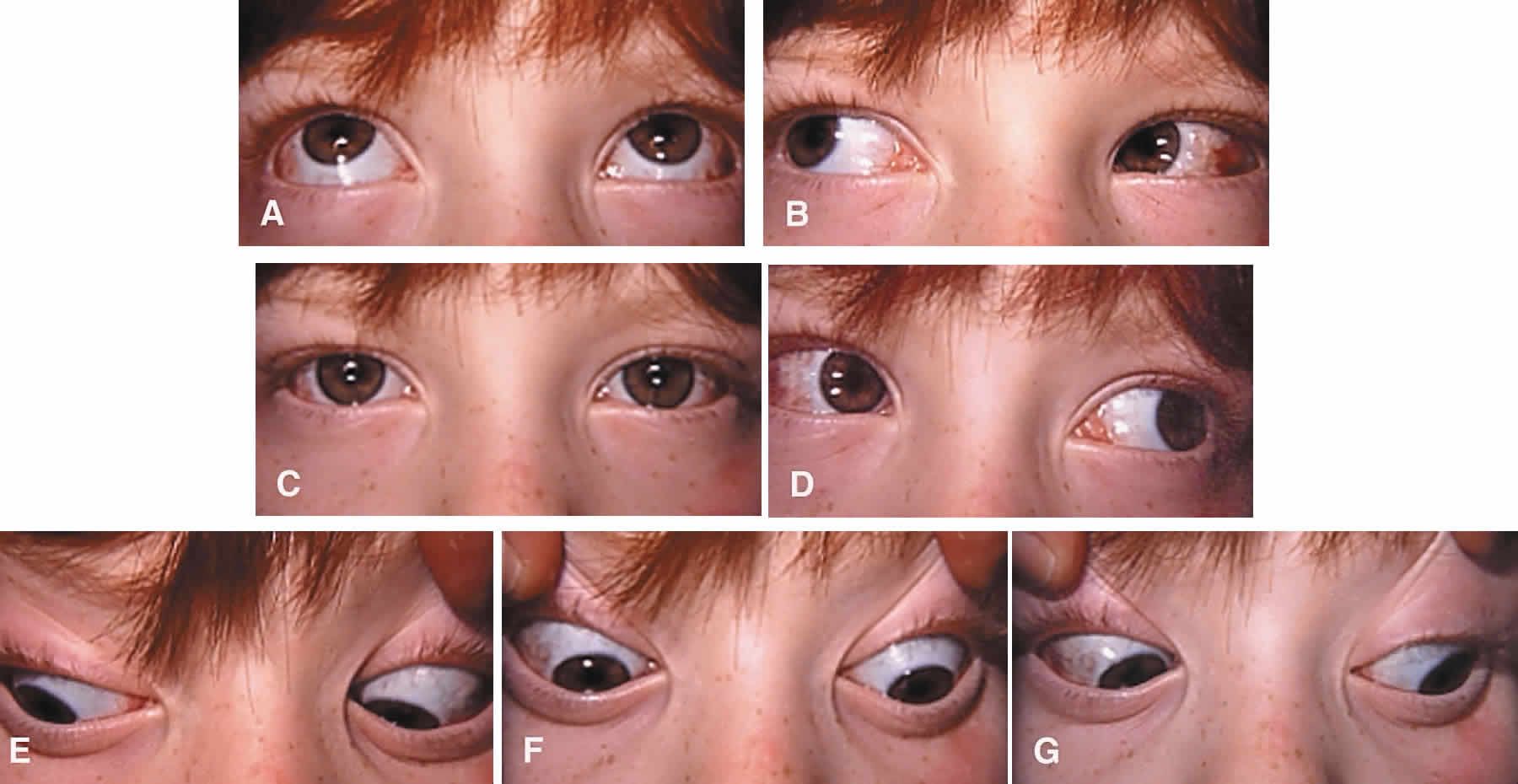
Surgery to correct unilateral, congenital superior oblique muscle palsy is the single most common indication for superior oblique muscle strengthening. It has traditionally been thought to be caused by dysfunction of the fourth (trochlear) cranial nerve. Patients typically present with an incomitant hypertropia characterized by elevation of the affected eye in adduction and overaction of the ipsilateral inferior oblique muscle. Diagnosis is normally supported (but not “diagnosed”) using Parks' three-step test.13 Compensatory torticollis is present in approximately 75% of cases, with the face turn or head tilt toward the opposite shoulder.14,15 This is often first noted when the child begins to walk. However, the presence of a vertical deviation in primary gaze position may be overlooked if the physician fails to evaluate ocular alignment with the child's head held erect. Chronic torticollis can result in asymmetric facial development and postural plagiocephaly (Fig. 1).16–18 Some authors believe that proper head positioning during sleep is more important than performing early surgery in preventing the facial asymmetry.19 It is not known whether early strabismus surgery can prevent or reverse this deformity.
|

Bilateral superior oblique muscle palsy occurs most commonly after head trauma and affects all ages. In children, bilateral superior muscle palsy is much more common than unilateral palsy and may be occult.20–22 However, primary overaction of the inferior oblique muscles is common in strabismic children and may be a source of diagnostic confusion. This latter entity can usually be distinguished from bilateral superior oblique muscle palsy by its association with horizontal strabismus (usually esotropia) in primary gaze position, a large V-pattern (which is most pronounced between primary position and up gaze), and a negative result to Bielschowsky's head tilt test. Although bilateral superior oblique muscle palsy may also present with a V-pattern, it is usually smaller in magnitude and characterized by an esotropia in down gaze rather than an exotropia in up gaze. These patients often adopt a compensatory chin-down position to facilitate fusion.
The preoperative diagnosis of bilateral superior oblique muscle palsy can be confirmed with intraoperative traction testing or direct assessment of superior oblique tendon laxity after surgical retrieval.23,24 Clinically subtle, bilateral superior oblique muscle palsy can usually be distinguished from a strictly unilateral palsy by a smaller than expected hyperdeviation in primary gaze position accompanied by reversal of the hypertropia in the field of action of the apparently normal superior oblique muscle or on Bielschowsky's head tilt test. Assessing the oblique fields of gaze for a reversal of the hypertropia is essential to detecting bilaterality in some cases.22 If closed head trauma can be excluded by history, the diagnosis of congenitally absent or hypoplastic superior oblique muscles or tendons (alone or combined) should be considered, especially in patients with other craniofacial anomalies.1 Imaging studies may demonstrate attenuation or absence of the superior oblique muscle.25,26
Treatment for congenital superior oblique muscle palsy can generally be delayed until after infancy. This is fortunate, because reliable prism and cover measurements are difficult to obtain in young children. Fusion is usually preserved in children who exhibit torticollis, and the risk of developing suppression and amblyopia is low.14 Patients with trochlear nerve injury from closed head trauma or other forms of reversible superior oblique muscle palsy should not be surgically treated for at least 6 months after onset or until spontaneous improvement has ceased.
Three main indications for corrective surgery exist: asthenopia, a manifest vertical strabismus in primary gaze or reading positions, and compensatory torticollis. Large vertical vergence amplitudes to maintain fusion are typically present in patients with long-standing deviations of several years or more. However, motor fusional effort may cause asthenopic symptoms. Alternatively, patients may complain of loss of binocular vision, a cosmetically objectionable hypertropia, or vertical diplopia when their deviation is manifest. Compensatory torticollis is common and often the primary reason for ophthalmologic consultation in children. Older children and adults with acquired, bilateral superior oblique muscle palsy may complain of torsional diplopia in the absence of vertical strabismus when forced to look down or use bifocal glasses. Cyclodeviation may also be noted in acquired vertical strabismus caused by restrictive ophthalmopathy or myasthenia gravis.27 Adaptations to tilting of the visual environment can occur in patients with acquired cyclotropia but are more deeply rooted in patients with congenital cyclotropia.28
To choose an appropriate operation, it is usually necessary to quantitate the vertical and horizontal alignment defects using prism and cover measurements or Maddox rod testing. When possible, these measurements should be obtained in the diagnostic gaze positions at distance and the near reading position. This task is time consuming but worthwhile, given that these measurements will determine the type and amount of surgery performed. In addition, important ancillary information can be obtained, such as the strength of vertical vergence amplitudes, a clinically significant horizontal deviation, or the presence of occult bilateral involvement. Assessment of subjective ocular torsion using the double Maddox rod or objective excyclotropia by fundus examination is often helpful in determining the surgical approach to be taken.
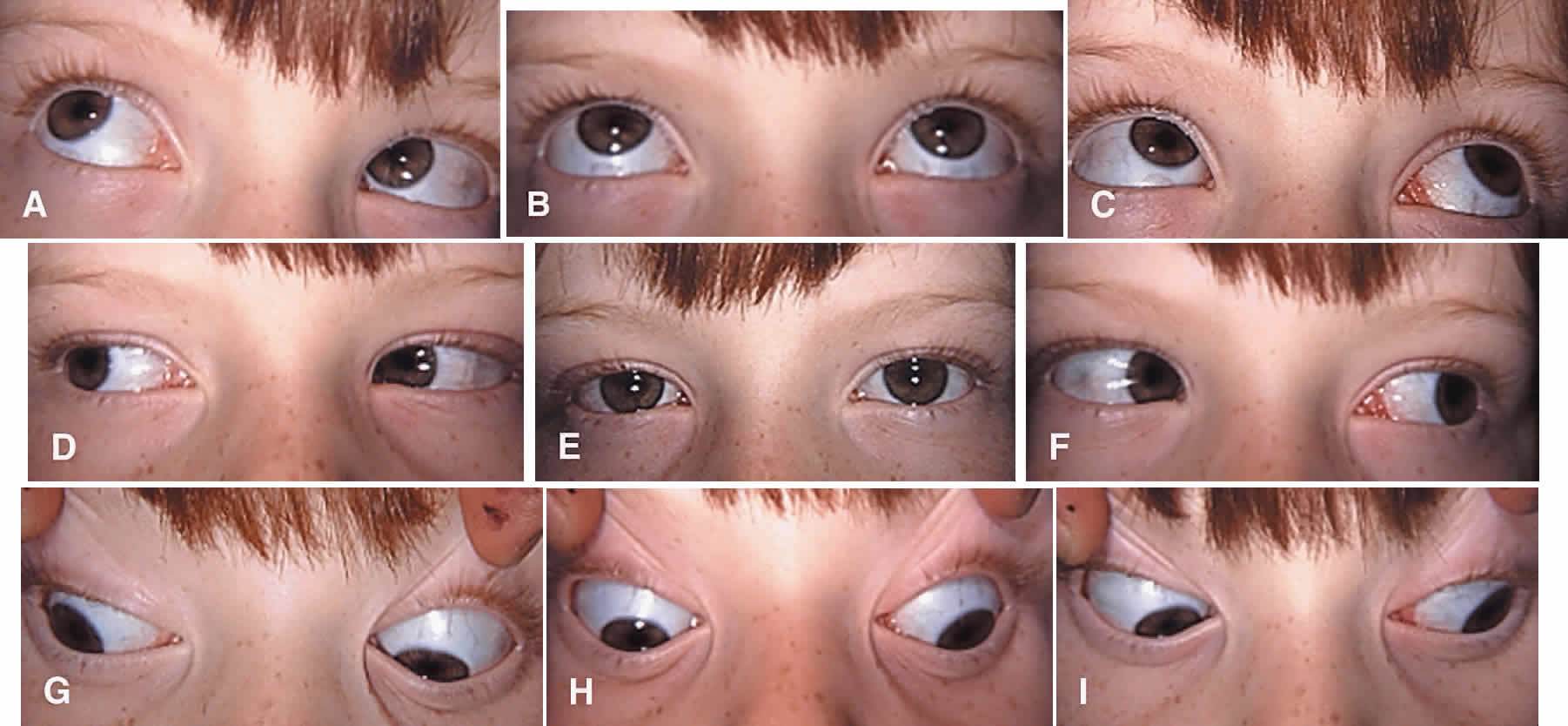
Successful results can be achieved with various surgical approaches (Fig. 2).29–36 Superior oblique muscle strengthening operations are usually performed in conjunction with surgery on other cyclovertical muscles. Their most common uses are (1) to augment ipsilateral inferior oblique muscle weakening in patients with at least 30 diopters (D) of hypertropia in lateral gaze or 20 D of hypertropia in primary gaze; (2) to augment ipsilateral superior rectus or contralateral inferior rectus muscle recession or posterior fixation in patients with increased hypertropia in down gaze; (3) to correct excyclotropia in the presence of a small hypertropia in primary gaze position; and (4) to improve the function of a congenitally lax or redundant tendon.37 In fact, torticollis may be difficult or impossible to eliminate in some children without a superior oblique tendon tuck or similar strengthening procedure.38 The Harada-Ito procedure and its modifications enhance intorsion and are used to correct excyclotropia when little or no vertical misalignment in primary gaze position exists.39–41 Its use, therefore, is limited primarily to correcting torsional diplopia in patients with bilateral superior oblique muscle palsy. Small horizontal deviations associated with superior oblique muscle palsy tend to resolve spontaneously after vertical realignment of the eyes. In our experience, concurrent horizontal rectus muscle surgery often (and for unknown reasons) leads to overcorrection and is usually unnecessary.
|

Superior oblique muscle strengthening is occasionally performed as an isolated procedure, often after surgical undercorrection following inferior oblique muscle weakening. Indications for this approach are persistent torticollis associated with a small residual hypertropia, excyclotropia, and clinical underaction of the paretic superior oblique muscle. A superior oblique tendon tuck is an appropriate primary procedure in patients with less than 10 D of hypertropia in primary gaze position, at least 5 degrees of subjective extorsion, and little or no overaction of the ipsilateral inferior oblique muscle. This situation is normally found in unilateral or bilateral posttraumatic superior oblique muscle palsy. Finally, patients with direct trauma to the superior oblique tendon after penetrating injuries of the upper eyelid and orbit may have a repairable injury and should have the superior portion of the globe carefully explored and severed portions of the tendon reapproximated if technically feasible.42
CONTRAINDICATIONS
Contraindications to superior oblique muscle strengthening are few, but important. Patients with small-angle, vertical deviations of less than 10 D in the fields of action of both the ipsilateral superior oblique and inferior oblique muscles and no torsional symptoms are not good candidates for superior oblique muscle strengthening procedures but can sometimes be managed successfully with prism-fitted glasses. However, prisms are rarely appropriate in children. Patients with preoperative underaction of the ipsilateral inferior oblique muscle or concurrent Brown's syndrome following trochlear injury should not undergo any procedure that could further compromise elevation of the eye. Similarly, the presence of a taught superior oblique tendon identified at the time of surgery, either by traction testing or direct inspection, should be a cause for concern. Such patients develop symptomatic postoperative Brown's syndrome following after minimal shortening of the superior oblique tendon.23,37,43–45 (Our only tuck takedown over 2 decades was required in a patient with posttraumatic superior oblique muscle palsy who had only 4 mm of tendon tuck performed!) Finally, the absence of excyclotropia or vertical incomitance in lateral gaze should prompt the surgeon to consider operating on alternative muscles. This is because superior oblique muscle strengthening typically produces between 5 and 10 degrees of intorsion in primary gaze position and has its greatest vertical effect in ad-duction. Although clinically important postoperative Brown's syndrome is uncommon, many patients have a mild, long-term elevation deficiency in the operated eye, particularly if the ipsilateral inferior oblique muscle has also been weakened. They often report vertical diplopia in extreme up gaze, which might pose problems in certain occupations (e.g., pilot, auto mechanic) or athletic activities requiring a full visual field of single binocular vision. Surgeons who lack full understanding of the patient's motility problem or who are insecure about their approach to the superior oblique tendon should not undertake superior oblique muscle surgery.
SURGICAL PROCEDURES
The superior oblique tendon tuck is the most frequently performed superior oblique muscle strengthening procedure. It is almost always performed unilaterally in patients with congenital superior oblique muscle palsy or acquired paresis in which marked tendon laxity is demonstrated by intraoperative traction testing.23,24 Although technically more difficult than tendon tucking, superior oblique tendon plication, advancement, or resection may be used in lieu of a tuck.46 In cases of acquired superior oblique muscle palsy in which tendon laxity is not present, the preferred surgical approach generally involves weakening the antagonist inferior oblique muscle or other vertical rectus muscles. The Harada-Ito procedure is usually performed bilaterally and is generally reserved for patients with acquired, bilateral superior oblique palsy to correct torsional diplopia.44
Tendon Tuck
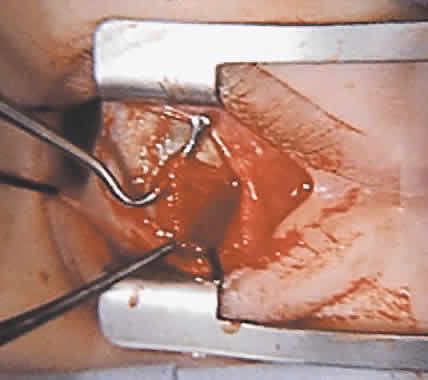
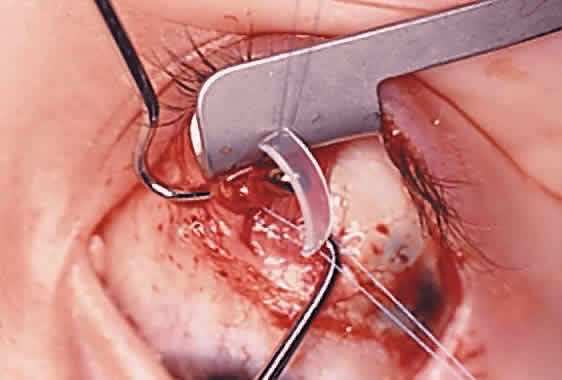
To perform the procedure, either general anesthesia or local anesthesia with intravenous sedation may be selected. Following anesthesia, it is often helpful to assess tendon laxity by performing an exaggerated traction test.47 A normal superior oblique tendon can be differentiated from a lax tendon when the globe is rotated upward, inward, and retropulsed into the orbit (Fig. 3).23
|
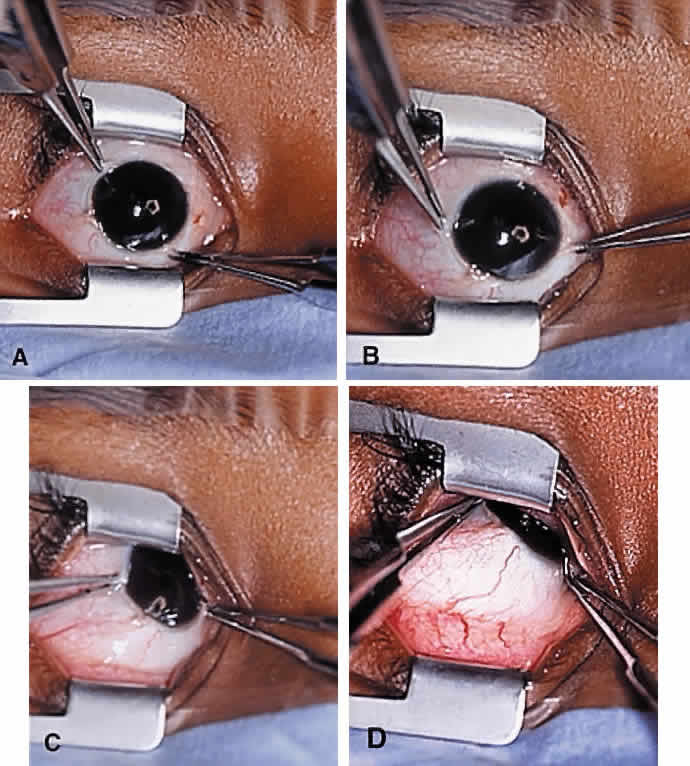
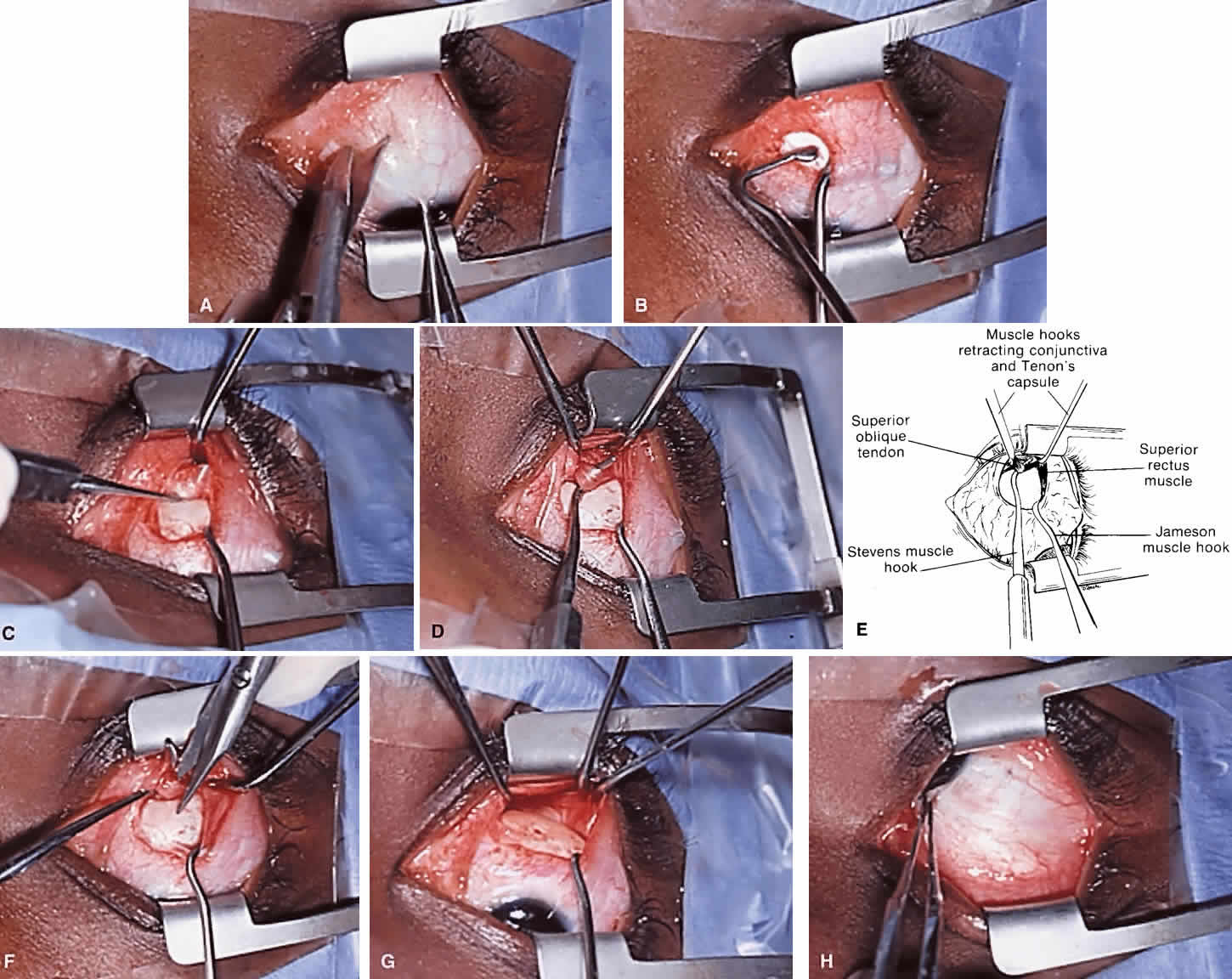
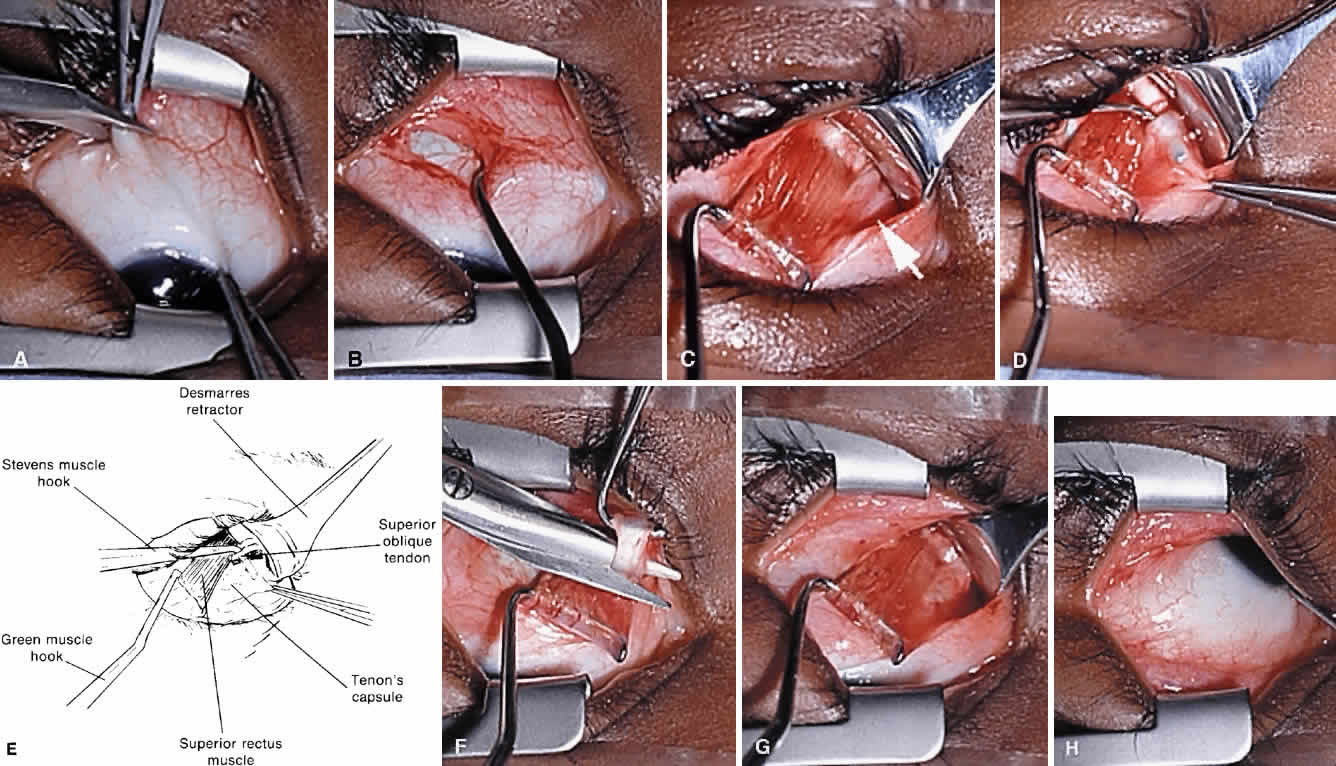
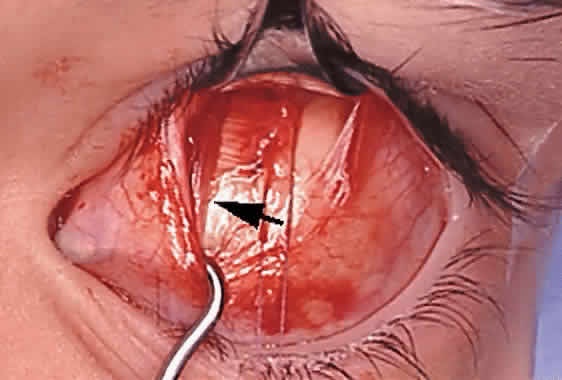
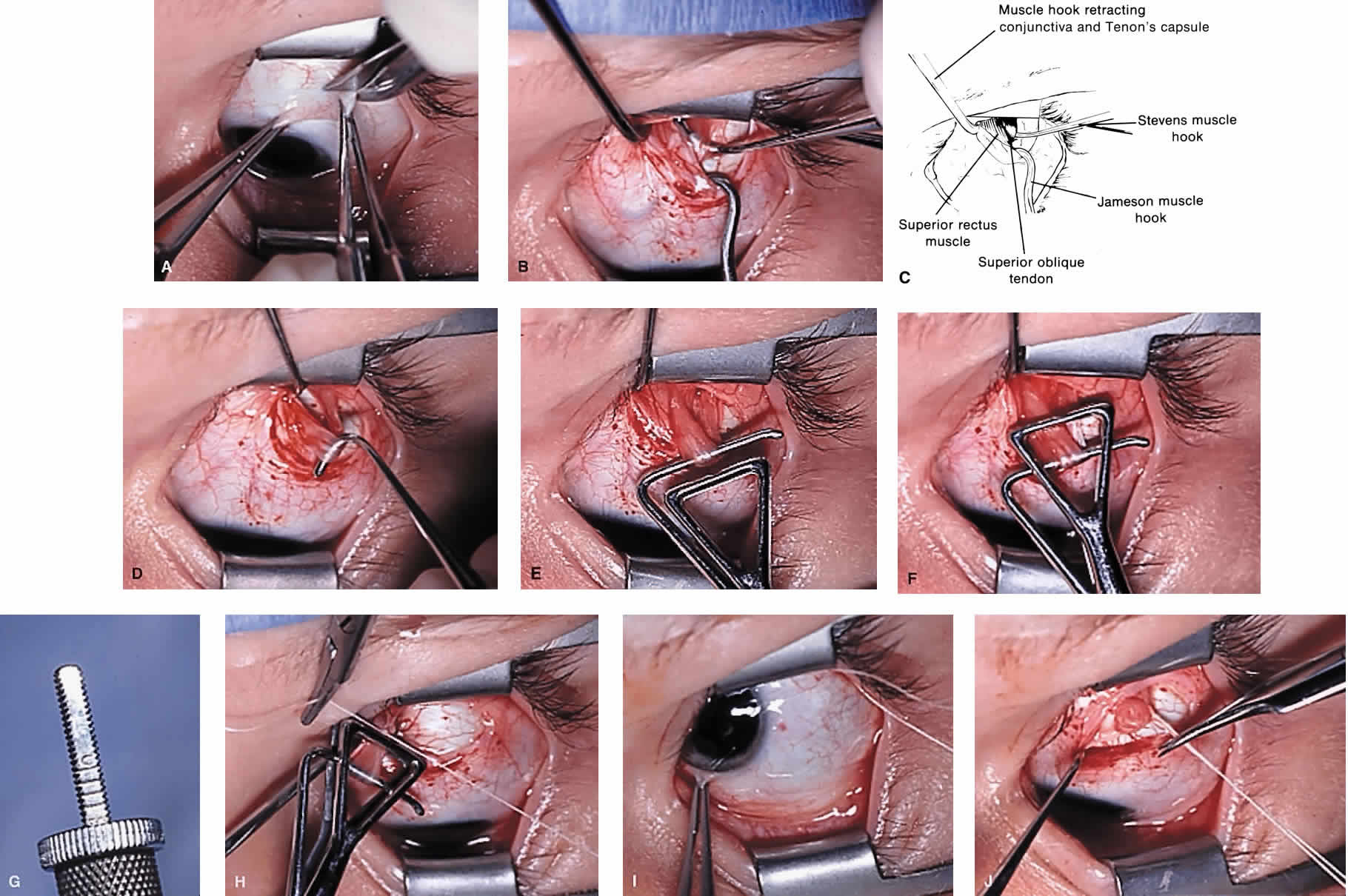
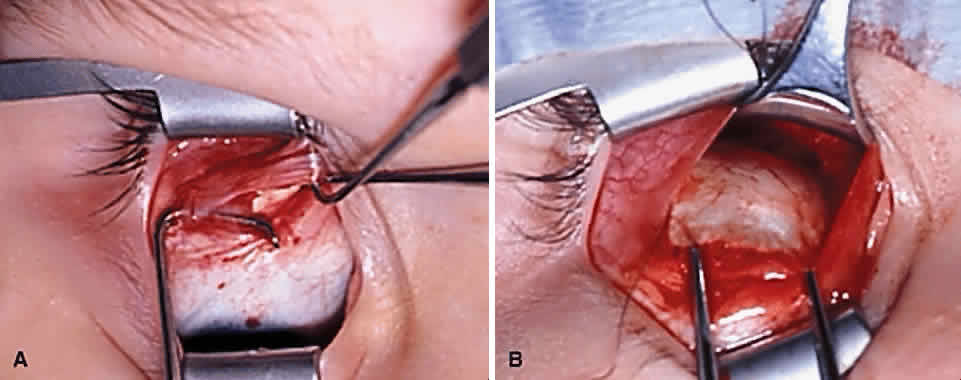
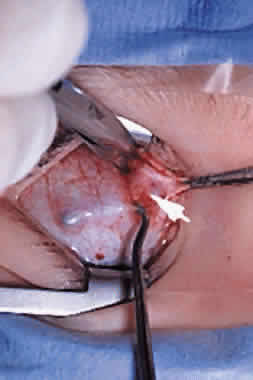
The superior oblique tendon tuck is best performed near the tendon's insertion as described by McLean.48 The surgical procedure is performed through a superior temporal cul-de-sac approach (Fig. 4). With the globe depressed, an incision is made through the conjunctiva and Tenon's fascia just temporal to the lateral border of the superior rectus muscle and parallel to the corneoscleral limbus. The superior rectus muscle is engaged on a muscle hook and the globe adducted and positioned in maximal depression. The lateral rectus muscle may also be used to assist positioning the globe. Using two small muscle hooks, the conjunctival incision is stretched open posteriorly in a triangular fashion. The lateral border of the superior rectus muscle is elevated and displaced medially. The globe is then examined for the glistening, white fibers of the superior oblique tendon running flush against the sclera and directed anteromedially. The anterior portion of the reflected tendon typically inserts under the lateral border of the superior rectus muscle, 5 to 7 mm posterior to its insertion. However, this location may vary, and anatomic anomalies are common (Fig. 5).12,37,47,48 The superior oblique tendon looks very different near its scleral insertion than 10 mm more proximally, where it becomes cordlike and enters Tenon's fascia after passing under the belly of the superior rectus muscle. Inexperienced surgeons have mistaken the lateral portion of the tendinous insertion of the superior rectus muscle for the superior oblique tendon (Fig. 6).49 However, the superior rectus muscle travels toward the orbital apex and contains prominent anterior ciliary blood vessels, whereas the superior oblique tendon is directed toward the trochlea and is usually avascular. In addition, direct traction on the superior oblique tendon can easily be palpated at the trochlea by pressing a finger over the eyelid in the superior nasal quadrant of the orbit.10 This is a reliable sign that the tendon (and not some other structure) has been engaged on the muscle hook.
|
|
|
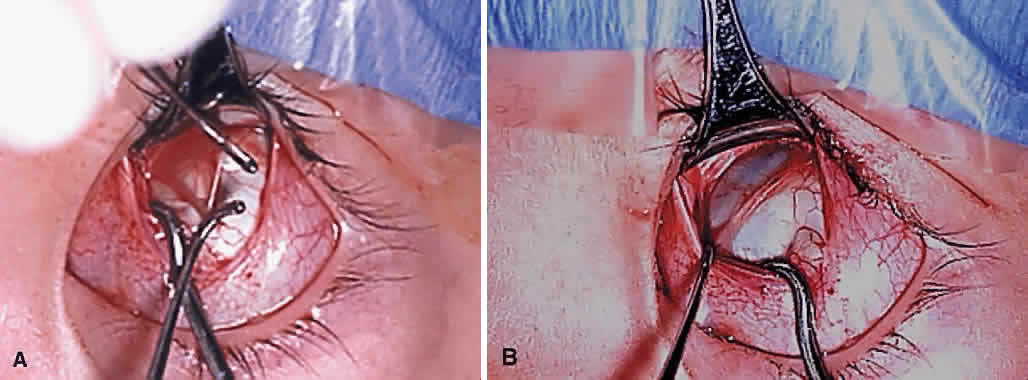
After the superior oblique tendon has been positively identified, it is gathered on a Stevens tenotomy or other muscle hook with a small tip. This maneuver is most readily accomplished by passing the hook over the tendon with its tip parallel to the sclera and pointed medially. Direct visualization of the tendon is essential, in that blind sweeping can be hazardous. A superior temporal vortex vein usually exists near the posterior insertion of the superior oblique tendon and the optic nerve is within reach. In addition, it is important to avoid passing the muscle hook into orbital fat because its release into the sub-Tenon's space predisposes the eye to develop an adherence syndrome postoperatively.50
The superior oblique tendon is drawn forward through the surgical wound and attachments to Tenon's fascia and the superior rectus muscle are cut. A second pass of the muscle hook helps ensure that no fibers have been missed. Gross assessment of tendon laxity is then performed. A lax tendon requires a greater amount of tuck, whereas a normal tendon should be approached with caution, and a taut tendon should not be shortened at all. A Bishop tendon tucker is helpful to control the isolated tendon and permits the surgeon to quantitate the amount of tendon shortening conveniently. The tendon is drawn in the tucker until snug, but not tight. The loop of tendon is then sewn to itself using a nonabsorbable suture such as 5-0 braided Dacron. After this provisional tuck has been completed, the tendon is released into the orbit and a traction test is performed with the eye positioned in maximum adduction. It has been our experience that the ideal tuck results when the amount of tendon shortening produces its first resistance to elevation as the inferior limbus crosses an imaginary line between the medial and lateral canthus (Fig. 7).34,51 Care must be taken not to retropulse the globe into the orbit, because this exaggerates the duction limitation. An average tendon shortening of approximately 12 mm is required in congenital superior oblique muscle palsy (lax tendon) and 8 mm in acquired palsy (normal tendon). However, the optimum amount of tuck does not necessarily correlate with the size of the hypertropia in primary gaze position and intraoperative titration is essential. If the initial tuck is too tight or too loose based on results of traction testing, the tendon is retrieved from the orbit and the tuck is adjusted. The final tie-off is performed by passing the suture through and around the superior oblique tendon a second time after which it is tied securely. This minimizes the potential for tendon slippage through the tuck and provides additional security should a suture loop fail postoperatively. It is not necessary to sew the redundant tendon to the sclera. Conjunctival closure is performed at the surgeon's discretion. A running suture of 6-0 plain catgut is well tolerated and prevents the conjunctiva from gaping open postoperatively.
|
Tendon Plication/Imbrication
This procedure is similar to the superior oblique tendon tuck, except that a nonabsorbable suture is secured to the tendon 6 to 9 mm from its insertion and then passed through the sclera just beyond the insertion. Pulling these sutures tight folds the tendon over onto itself (“imbrication”) and advances the midportion of the tendon.46 Plication shares reversibility with the superior oblique tendon tuck, although it alters the normal anatomic insertion of the tendon and is more difficult to adjust intraoperatively.
Tendon Resection/Advancement
The superior oblique tendon can be resected or advanced in a manner similar to that used for rectus muscles (see Fig. 2C). However, the long and fanlike tendinous insertion makes this technique more challenging, even with optimal exposure, and typically results in narrowing and some anterior transposition of the scleral insertion. Furthermore, this procedure is less easily reversible than superior oblique tendon tuck and other nondisinsertion procedures. Therefore, superior oblique tendon resection is rarely, if ever, selected by most surgeons.
Harada-Ito Procedure
The Harada-Ito procedure is usually indicated in patients whose primary complaint is torsional diplopia (Fig. 2E, F and Fig. 8). This is encountered most often in adult patients with bilateral, posttraumatic superior oblique muscle palsy. Patients with congenital superior oblique palsy often have sensory adaptations that partially or completely compensate for years of excyclotropia. Although used primarily to correct symptomatic excyclotropia in patients with little or no vertical deviation in primary gaze position, it may also be effective in the treatment ocular torticollis with tilt-dependent nystagmus.52,53 The Harada-Ito procedure involves selective strengthening of the anterior fibers of the superior oblique tendon that are primarily responsible for incyclotorsion. It can be performed either by disinserting, advancing and anteriorly transposing the anterior tendon fibers (disinsertion technique) as described by Fells54 or by the classic Harada-Ito method, which redirects the anterior fibers as a “dog leg” without scleral disinsertion (Fig. 8).40 We prefer the classic method because it is more easily reversible. However, the disinsertion technique has the advantage of being readily modified for use with adjustable sutures.41,55 Superior oblique tendon tuck limited to the anterior fibers is an occasionally useful alternative when an intermediate amount of incycloduction is desired with some vertical correction.
|
To perform the classic Harata-Ito procedure, the superior oblique tendon is identified and isolated on a muscle hook in a fashion similar to a superior oblique tendon tuck (see previous discussion). A small muscle hook is used to separate between one third and one quarter of the most anterior tendon fibers for approximately 8 to 10 mm from their scleral insertion. A nonabsorbable, double-armed suture, such as 5-0 braided Dacron, is passed through the tendon defect and then through the sclera adjacent to the superior border of the lateral rectus muscle posterior to its scleral insertion. When the suture is secured to the sclera, the anterior fibers are advanced and anteriorly transposed to create a new functional insertion. The surgical effect can be titrated by altering both the tension and position of the suture using an intraoperative adjustment technique in cooperative patients or fundus examination under general anesthesia.56 Postoperative overcorrection can easily be addressed by cutting the scleral suture. If performed during the first several days after surgery, the transposed fibers of superior oblique tendon return to their normal anatomic position.
Tendon Transposition
Patients with a history of third (oculomotor) cranial nerve palsy and absent medial rectus muscle function often have persisting exotropia because of unopposed action of the ipsilateral lateral rectus muscle. If the vertical rectus muscles are paretic and transposition surgery is therefore inappropriate, the superior oblique muscle can be used as an adductor and elevator to stabilize the globe in primary gaze position. Jackson57 and later Costenbader58 suggested fracturing the trochlea and reattaching the superior oblique tendon to the sclera above the insertion of the medial rectus muscle. Scott subsequently described a simplification of this procedure, not involving trochleotomy, in which the reflected portion of the superior oblique tendon is disinserted from the sclera, rotated anteriorly, and reattached adjacent to the medial border of the superior rectus muscle.59 Some authors have reported favorable results when the superior oblique tendon transposition is accompanied by aggressive horizontal rectus muscle surgery,60 whereas others have found it less effective or accompanied by unacceptable paradoxical ocular movements.61
Expected Results
After tucking the superior oblique tendon, most patients have a mild-to-moderate elevation deficiency in adduction (Brown's syndrome).62 Elevation deficiency may be less pronounced after superior oblique tendon advancement or resection. Patients undergoing the Harada-Ito procedure do not characteristically have elevation defects in adduction postoperatively but may report subjective extorsion with corresponding incyclotropia on fundus examination.63 Following any shortening procedure of the superior oblique tendon, there may be tenderness in the trochlear region and avoidance of elevation in adduction.
When surgery for superior oblique muscle palsy is limited to one or more oblique muscles, a small overcorrection of less than 10 D is desirable in primary gaze position. Because results of Bielschowsky's head tilt test usually remains positive postoperatively, many patients temporarily adopt an opposite head tilt toward the side of the paretic muscle or a chin-up head posture to avoid diplopia or achieve fusion. If the patient wears glasses, a base-up Fresnel prism over the operated eye may be helpful during the early postoperative period. Surgical overcorrection, especially following treatment for a large-angle, congenital superior oblique muscle palsy, should not be reoperated hastily and rarely within 1 year. Almost all such patients improve spontaneously. Similar to the surgical treatment of intermittent exotropia, long-term undercorrection is much more common than permanent overcorrection. However, the surgeon should attempt to distinguish between a true surgical overcorrection and masked, bilateral superior oblique muscle palsy, which is likely to require additional treatment.17,20–22,64
Because of the heterogeneous nature of this population and differences in inherent prognosis, meaningful reoperation rates are difficult to calculate. Most patients undergoing superior oblique tendon tuck for appropriate indications will not require a second surgery. Successful outcomes (elimination of torticollis and manifest hypertropia in and around primary gaze position) may be as high as 90%.16,36,44,51 In general, patients with congenital or long-standing superior oblique muscle palsy characterized by inferior oblique muscle overaction and near normal superior oblique function have the best prognosis, regardless of the magnitude of the deviation in primary gaze position. Patients with bilateral or posttraumatic superior oblique muscle palsy tend to fare less well, perhaps because of poor vertical vergence amplitudes or limited fusion capability. It is likely (but unproven) that patients with partial superior oblique muscle dysfunction (paresis) have a better surgical prognosis than those with complete paralysis. Because the treatment indication for superior oblique tendon anterior transposition is third cranial nerve palsy rather than superior oblique muscle palsy, the expected surgical results should be considered separately. Although enhancing adduction forces on the eye may help stabilize the globe in primary gaze position, paradoxical adduction on attempted depression may be an undesired result.61 The tethering effect of the superior oblique tendon may also produce globe elevation in abduction.
COMPLICATIONS
Serious complications of superior oblique muscle strengthening are infrequent. Intraoperative complications relate primarily to orbital hemorrhage from injury to a vortex vein or unintended entry into the orbital fat space, which results in an adherence syndrome with restricted ductions postoperatively. These can be avoided by good surgical exposure, use of loupe magnification with a surgical headlight, and deliberate and meticulous surgical technique. The superior oblique tendon can be surgically missed or inadvertently cut during dissection of the intermuscular septum. Anatomic variations including absence of the tendon are common.12 Confusion can also occur if the surgeon inadvertently engages the superior oblique tendon when first attempting to hook the superior rectus muscle.49 However, this is less common when the superior oblique tendon is approached temporally rather than nasally (Fig. 9). Surgical overcorrection occurs frequently, but it is fortunately not permanent in most patients. However, permanent overcorrection that results in a primary gaze position hypotropia is usually an unacceptable result and requires reoperation. It can be caused by excessive surgical dosage, spontaneous recovery of superior oblique muscle function, or failure to recognize bilateral superior oblique muscle palsy preoperatively.
|
Iatrogenic Brown's syndrome is an unavoidable complication of superior oblique muscle strengthening and occurs in almost 100% of patients undergoing superior oblique tendon tuck. It is virtually identical in clinical appearance to congenital Brown's syndrome, which is discussed later in this chapter (Fig. 10). In the absence of excessive tendon shortening, the limitation of elevation in adduction almost always improves with time and reoperation for this entity is rarely required. Tendon tucking medially (rather than temporally) to the superior rectus muscle is more hazardous because of proximity to the trochlea. Patients with persisting overcorrection in primary gaze position and at least moderate Brown's syndrome (no elevation above the horizontal meridian in adduction) are usually symptomatic and should have their tucks removed. However, adhesions between the superior rectus muscle, superior oblique tendon, and the globe are likely to be present and must be freed to normalize ductions. In general, tuck take down should be performed without simultaneous surgery on other cyclovertical muscles.
|