|
| Chapter 61 Trauma: Ruptures and Bleeding EARL R. CROUCH, JR and ERIC R. CROUCH Table Of Contents |
|
TRAUMA TO THE UVEAL TRACT TRAUMA TO THE IRIS IRIDODIALYSIS TRAUMA TO THE CILIARY BODY TRAUMATIC HYPHEMA TRAUMA TO THE SCLERA TRAUMA TO THE CHOROID REFERENCES |
| TRAUMA TO THE UVEAL TRACT |
| Blunt ocular trauma frequently causes injury to the uveal tract.1,2,3 Injury to the uvea may be either direct or contrecoup. The sudden, transient increase of intraocular pressure (IOP) following impact is probably insufficient to produce much of the damage usually encountered. One possible mechanism of injury is direct contusion of the cornea, which produces a marked posterior displacement, first of the cornea and then of the iris-lens diaphragm. This places great stress on the area of the iris root and on the zonules attached to the ciliary body. In addition, the sclera expands in circumference in the area of the ciliary body. The ciliary body follows suit; however, its greater mass causes a lag in expansion, with possible subsequent separation within the uveal tissues or between the ciliary body and the sclera.1,4,5 An alternative explanation for damage is the creation of a pressure wave that travels posteriorly within the aqueous. As the pressure wave strikes the lens, it is directed laterally and circumferentially, which results in a concentration of its force at the iris root. |
| TRAUMA TO THE IRIS |
IRITIS Traumatic iritis is the mildest result of blunt injury to the iris. Contusion injury to the iris stroma results in anterior chamber flare and cells; it is accompanied by aching, photophobia, and ciliary injection. Disruption of the blood-aqueous barrier may accompany blunt trauma. Traumatic iritis is occasionally accompanied by pain with direct illumination into the uninjured, contralateral eye.6 Topical treatment of cycloplegia produces symptomatic improvement, and spontaneous recovery is the rule. In more severe iritis, topical steroids provide comfort and hasten recovery. PIGMENTARY CHANGES Visible scattering of intraocular pigment almost always follows ocular trauma. A fine dusting of pigment may be observed on the corneal endothelium, trabecular meshwork, anterior lens capsule, iris surface, and occasionally in the vitreous. Small clusters of dense pigment may remain on the stromal surface of the iris, indicating previous hyphema.7 A Vossius lenticular ring may give additional evidence of ocular trauma. A Vossius ring is a full or partial circle of pigment deposited on the anterior capsule of the lens, corresponding to the pupillary margin. It is usually noted after dilation of the pupil with mydriatics. This imprint of iris epithelial pigment is probably deposited on the lens surface as the aqueous pressure wave momentarily compresses the pupillary margin of the iris against the lens. The Vossius ring usually disappears with time. Occasionally, remnants may remain permanently on the anterior surface of the lens. HEMORRHAGE Hemorrhage into the iris stroma is an infrequent posttraumatic finding. The vessels in the iris stroma have the capacity to retract and close spontaneously. Therefore, hemorrhage within the iris stroma is usually confined to very small areas that rapidly turn brown or totally disappear. SPHINCTER ALTERATIONS Miosis and Mydriasis The response of the iris and the ciliary body to concussive force may be either irritative or paralytic. A mild concussion may cause a traumatic miosis and spasm of accommodation. Miosis may also accompany a posttraumatic iritis. More serious injury may cause a traumatic mydriasis and cycloplegia. Mydriasis and miosis are usually short lived and improve spontaneously. The ciliary and iris muscles are usually affected simultaneously; however, iridoplegia may be present without impairment of accommodation. Iris stromal tears may appear centrally as sphincter damage or peripherally at the iris root as iridodialysis. Sphincter Rupture Rupture of the iris sphincter is sometimes produced by blunt trauma. Single or multiple tears in the iris stroma (with iris sphincter involvement) may cause small triangular defects or teardrop defects in the pupillary border. Anterior concussion causes the aqueous to press the iris against the lens, resulting in forced pupillary dilation as the pupil and sphincter are forced to dilate over the dome of the anterior lens capsule. With blunt trauma, the pupil dilates rapidly and may induce shearing forces in the sphincter pupillae. At the same time, there is reflex constriction of the pupillary sphincter. When the limits of elasticity of the iris stroma are reached, the weakest areas rupture. Part or all of the iris thickness may be involved. Small strands of anterior iris stroma may show separation; alternatively, only the posterior pigment epithelium and sphincter may be affected. Transillumination of the iris tissue is often required for recognition of the latter. Most frequently, all layers tear simultaneously, leaving a notch in the pupillary border or a triangular defect with its apex directed toward the iris root. Torn iris tissue is a permanent defect, because the iris is unable to repair its structure. IRIDOSCHISIS Blunt trauma may cause iridoschisis, that is, a portion of the anterior mesodermal leaf of the iris detaches from the posterior iris stroma or epithelium. The detached leaf of anterior stroma then floats forward into the anterior chamber. Alternatively, detached segments of the iris stroma may atrophy, leaving areas of thin, depigmented stroma or bare pigment epithelium. |
| IRIDODIALYSIS | |
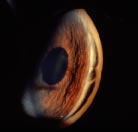
In iridodialysis, the base of the iris separates from the ciliary body
and scleral spur (Fig. 1).The iris root is the thinnest and weakest area of the iris. With severe
concussive injuries, a large sector of the iris root may tear free, creating
an accessory pupil of significant size at the limbus. This type
of injury may be associated with a large hyphema; therefore, the iris
injury may not be noted until the hyphema clears. The iridodialysis
seldom requires treatment, except when it causes symptomatic monocular
diplopia. Indeed, corrective measures should be deferred until the
vision is stable, because iridodialysis is frequently associated with
other, more serious injuries, which preclude good vision. Persistent diplopia
may be corrected by resuturing the iris with 10-0polypropylene
suture.8 For McCannel iris techniques, a longer needle such as Ethicon CIF-4 is
required.9 Various techniques have been employed to repair an iridodialysis with
a closed anterior chamber, using partial thickness scleral flaps similar
to those used for sulcus fixation of posterior chamber intraocular
lenses. The procedure should be undertaken with caution. There is the
potential to produce a recurrent hyphema, because the incision may have
to pass through a proliferative scar from the original injury.
|
| TRAUMA TO THE CILIARY BODY | |
ANGLE RECESSIONS Blunt contusion of the globe frequently causes damage to the anterior chamber angle, with or without bleeding into the anterior chamber.2 Concussive force produces a cleft in the ciliary body, usually between the circular and the longitudinal muscle fibers, beginning at the scleral spur. Less frequently, the cleavage may occur either more centrally in the circular muscle fibers or more peripherally, producing a cyclodialysis cleft. Minor angle damage may be recognized as a separation of the strands of the uveal meshwork.10,11 The recessed meshwork tends to be disrupted in its midportion, resulting in small tufts of uveal tissue bunching up on the iris root and on the trabeculum above the scleral spur. This leaves the ciliary body bare in comparison with other quadrants of the angle or with the angle of the opposite eye. With mild injuries of this sort the examiner should compare the gonioscopic appearance of both eyes simultaneously with two Koeppe lenses (compare two parts of the angle of one eye) to identify subtle changes in the injured angle. In more severe injuries, the cleft extends into the ciliary body. The light gray portion of the ciliary band appears broadened, and the scleral spur is more distinctly white and prominent. (Fig. 2) Small peripheral anterior areas of synechiae frequently appear at the lateral limits of an angle recession. In contrast, a cyclodialysis cleft, in which a sector of the ciliary body is totally detached from the sclera, is recognizable by the area of white sclera that is visible posterior to the scleral spur.
Although angle recessions may occur without anterior chamber hemorrhage, most patients have coexistent hyphemas. Careful gonioscopy has revealed that between 71%10 and 86%11 of traumatized eyes with hyphemas have an angle recession. The amount of angle recession is usually not related to the amount of hyphema; some small hyphemas had large, deep recessions, whereas some minor angle recessions were associated with large hyphemas.10 Angle recession is a frequent cause of unilateral glaucoma. Blanton12 described two posttraumatic periods of pressure elevation; these periods are exclusive of the initial elevation of IOP during the acute phase of the hyphema. The first period usually begins 2 months to 2 years after the injury. Ocular hypertension at this time is often related to the amount of angle recession and is difficult to control with medical therapy. This period of hypertension may last for several months to several years, and it frequently subsides spontaneously (provided a large portion of the angle is not obstructed by peripheral anterior synechiae). However, optic nerve damage may occur if hypertension is uncontrolled. Medical therapy, although it produces poor control at times, should be relied on to “weather” this early period of glaucoma. A late period of elevated IOP may occur 10 to 15 years after the injury. Eyes with recessions greater than 180 degrees are particularly prone to this late-occurring glaucoma; nearly all patient whose angle damage approaches 270 degrees to 360 degrees develop late elevations of IOP.12,13 The incidence of this glaucoma is approximately 7% in persons with angle recession. In addition, angle recession of any amount seems to further elevate IOP in an eye in which primary open-angle glaucoma has coincidentally developed. Thus, inadequate IOP control and glaucomatous damage may occur more frequently in an injured eye that has concomitant open-angle glaucoma and an angle recession. Patients with known blunt trauma should be examined gonioscopically for angle recession; if angle recession is found, they should be advised to have yearly examinations for the rest of their lives to detect late-occurring glaucoma.14 CYCLODIALYSIS Occasionally, the separation of the ciliary body attachment to the scleral spur occurs. Temporary or permanent hypotony can result. A cyclodialysis cleft should be suspected if IOP is less than 9 or 10 mm Hg. Occasionally, the full thickness of the ciliary body detaches from the sclera, producing a cyclodialysis cleft. Localization of the cyclodialysis cleft may be visualized with scleral transillumination, biomicroscopy, and ultrasound.15,16 Traumatic cyclodialysis may occur as a small or a wide cleft; either size cleft may result in low intraocular tensions that continue as long as the cleft remains open. Spontaneous closure of the cleft (or operative closure to correct hypotony) may produce rapid elevation of IOPs to dramatically high levels. Rarely, blunt trauma may produce complete ciliary and choroidal detachment, that is, 360 degrees. This allows the iris-lens diaphragm and ciliary body to shift markedly backward or forward, frequently resulting in hypotony and phthisis bulbi. |
| TRAUMATIC HYPHEMA | ||||||
| The accumulation of blood in the anterior chamber is one of the most challenging
clinical entities encountered by the ophthalmologist. Even a
small hyphema can be a sign of major intraocular trauma with associated
damage to other intraocular tissues. Blunt trauma causes anterior chamber
angle distortion that may result in iris or ciliary body vessel
rupture and bleeding into the anterior chamber. The lack of an ideal
therapeutic program, the potential for secondary hemorrhage, and the secondary
onset of glaucoma all threaten to turn an eye with an initially
good visual prognosis into a complex therapeutic problem with poor
final visual result. EVALUATION The patient with traumatic hyphema should have a thorough ophthalmologic evaluation. The time of onset and type of injury should be recorded accurately. The object producing the injury and the method by which it produced the injury give additional insight into the amount of ocular damage. If several days have elapsed since the injury, the onset of diminished visual acuity or an increase in ocular pain is significant, because they may indicate secondary hemorrhage and/or elevated IOP. Any other history of ocular problems, including amblyopia, should be recorded. The ocular examination should be thorough and include the surrounding tissues.13 One should resist the temptation to abandon the examination when one cannot see beyond the anterior chamber. The periorbital skin should be searched for areas of hypesthesia or anesthesia. Blow-out fractures frequently accompany hyphemas.13 The lids and conjunctiva should be examined carefully for laceration. Disproportionate conjunctival edema should be regarded as a possible indication of scleral rupture until proven otherwise. Proptosis may indicate retrobulbar hemorrhage; enophthalmos and/or restrictions in extraocular muscle rotations suggest a blow-out fracture. Visual acuity of both eyes with best optical correction should be recorded. If the acuity of the injured eye is markedly reduced, light projection and color sense should be tested including evaluations of consensual reaction of the pupil of the uninjured eye. (Inappropriately poor visual acuity suggests concomitant optic nerve or macular damage.) The cornea is examined for damage or pre-existing disease, because any compromise of the endothelium increases its susceptibility to blood staining. The amount and character of the hyphema as it first presents should be recorded. Careful drawing of the shape of the clot or of the level of free cells aids in evaluation of secondary hemorrhage or resolution of the hyphema. One should note iris and lens details that are visible beyond the hyphema, that is, pupillary size and shape, sphincter tears, iridodialysis, and dislocation of the lens or other injuries. Examination of the fundus should be attempted but may be difficult until the hyphema has resolved. The pupil should be dilated if one suspects intraocular foreign body, rupture or perforation of the globe, or retinal tears or detachment. In most instances, a fundus evaluation is preferred when the media are clear following resolution of the hyphema. IOP should be recorded by applanation tonometry. Topical anesthesia and facial akinesia may be required (this is helpful in uncooperative children or intoxicated adults) if lid squeezing prevents adequate examination. Avoid gonioscopy until day 14 to avoid a secondary hemorrhage. Many patients with hyphema appear somnolent. The exact mechanism for this reaction is not clear. If associated head trauma is possible, neurologic consultation and magnetic resonance imaging (MRI) should be obtained. Laboratory data should include platelet count, prothrombin time, and partial thromboplastin time (PTT). All black and Hispanic patients require a sickle cell prep and, if positive, hemoglobin electrophoresis. CHARACTERISTICS AND CLASSIFICATION Traumatic hyphema is most often encountered in children. Reports indicate a prevalence of 70% or greater in the pediatric population.17 Males are involved in three fourths of cases.11,17 Studies in the United States indicate that hyphemas occur in approximately 20 per 100,000 population per year.18 The agent producing a hyphema is usually a projectile that strikes the exposed portion of the eye. Sources of trauma have included balls, rocks, projectile toys, air-gun or BB pellets, paint ball pellets, and the human fist19–21 (Figs. 3 and 4). Fists and belts have started to play a prominent role in cases of child abuse. Sports injuries, including soccer, hockey, baseball, and basketball injuries, account for up to 60% of traumatic hyphemas, which in many cases are related to lack of protective eye gear.
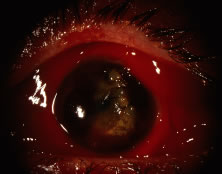
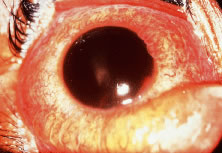
Rarely, spontaneous hyphemas may occur and be confused with traumatic hyphemas. Spontaneous hyphemas are secondary to neovascularization, ocular neoplasms including retinoblastoma and malignant melanoma, uveitis, and vascular anomalies (juvenile xanthogranuloma). Vascular tufts that exist at the pupillary border have been implicated in spontaneous hyphema.22 The level of hyphema has been classified into four grades, according to the amount of blood occupying the anterior chamber. Most hyphemas (58%) are classified as grade 1 (Fig. 5), meaning the hyphema consists of layered blood occupying less than one third of the anterior chamber. Microhyphema is a grade 1 hyphema. It is defined as a suspension of erythrocytes in the anterior chamber without formation of a layered clot. In grade 2 hyphema, blood fills one third to one half of the anterior chamber; 20% of hyphemas are classified as grade 2. Grade 3 hyphema is layered blood filling one half to less than the total anterior chamber, and 14% fall into this grade. Grade 4 is the least commonly occurring (8%) hyphema (Fig. 6), and it is defined as a total clotted hyphema, often referred to as blackball or eightball hyphema.
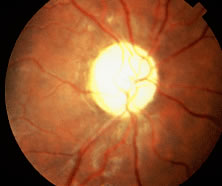
Slightly fewer than half of all hyphemas settle inferiorly to form a level. Approximately 40% form a definite clot, usually adherent to the iris stroma; 10% have a dark clot in contact with the endothelium.11 The source of anterior chamber hemorrhage in contusion injuries is thought to be related to the displacement of tissues posteriorly or to the resultant fluid wave in the aqueous and vitreous, which stretches the limbal vessels and displaces the iris and lens. This usually results in a tear at the iris or ciliary body, usually at the angle structures.12,21 A tear at the anterior aspect of the ciliary body is the most common site of bleeding and occurs in about 71% of cases.11,18 The blood exits from the anterior chamber via the trabecular meshwork and Schlemm's canal or the juxtacanalicular tissue. The usual duration of the uncomplicated hyphema is 5 to 6 days. ELEVATED INTRAOCULAR PRESSURE Increased IOPs may accompany hyphemas of any size. Elevated IOPs (above 24 mm Hg) may be anticipated in approximately 24% to 32% of all hyphema patients at some time during their first 7 days of treatment.11 Higher, more prolonged elevations of IOP are more commonly associated with near total or total hyphemas. The types of glaucoma in hyphema have a variety of mechanisms. The pathogenesis of the glaucoma related to erythrocytes in the anterior chamber includes a trabecular blockage with normal or sickle erythrocytes. Pupillary block glaucoma occurs as a result of large hyphemas. Glaucoma not related to the erythrocytes in the anterior chamber includes angle recession glaucoma, involving greater than 180 degrees of the trabecular meshwork. More than 270 degrees of angle recession definitely indicates significant long-term glaucoma. Blanton12 described two periods of elevated IOP, between 2 months and 2 years after the injury and 10 to 15 years after the injury. The amount of angle recession is not related to the amount of hyphema. Some small hyphemas produce large, deep recessions. In traumatic hyphema, if 180 degrees or more angle recession is found, the patient needs periodic examinations to detect late-occurring glaucoma.12 Glaucoma related to peripheral anterior synechiae occurs after 9 days of blood in the anterior chamber.12 Posterior synechiae with iris bombé may also occur. These highly elevated IOPs occur during the acute phase of the hyphema and are separate from those related to angle recession.11,12 In patients with pressure elevations, abnormal tonometric readings are frequently detected during the first 24 hours after injury. This initial period of elevated IOP is often followed by a period of normal or below normal pressure from the second to the sixth day. The early period of elevated IOP is the result of trabecular plugging by erythrocytes and fibrin. The following period of reduced pressure is most likely due to reduced aqueous production. A period of hypotony is commonly followed by a subsequent rise in IOP with the recovery of the ciliary body. In traumatic hyphema, control of elevated IOP is important to prevent complications of optic atrophy and corneal blood staining. Exceptions to this are those patients with hyphema occupying greater than 75% of the anterior chamber and patients with total hyphema, in whom pressure elevation frequently has its onset simultaneously with the initial hyphema and remains continually elevated until the hyphema has had considerable resolution. When large segments of the anterior chamber angle are irreparably damaged and/or when organization of the fibrin or clot produces extensive peripheral anterior synechiae, the intraocular hypertension continues, becoming intractable glaucoma. Ghost cell glaucoma with hyphema and vitreous hemorrhage may cause elevation of IOP 2 weeks to 3 months after initial injury.23 There is gradual clearing of the hyphema with erythrocytes losing hemoglobin and becoming so-called ghost cells in the vitreous cavity. The ghost cells then press forward into the anterior chamber, with resultant later elevation of IOP. SECONDARY HEMORRHAGE Secondary hemorrhage occurs in approximately 22% of all hyphema patients, with a range between 6.5% and 38%.10, 18, 21, 23, 24, 25, 26, 27, 28, 29 The incidence of secondary hemorrhage is higher in grade 3 and 4 hyphemas.21 Two reports indicate a higher rate of secondary hemorrhage in pediatric patients younger than 6 years.11,24 Frequently there is a relationship between child abuse and hyphema in this younger age group. Secondary hemorrhage usually occurs on the third or fourth day, but it may occur from the second to seventh day after trauma.11 Secondary hemorrhage is due to lysis and retraction of the clot and fibrin aggregates that have occluded the initially traumatized vessel. One third of all secondary hemorrhages proceed to total hyphema. In patients with a total hyphema at onset, in which the blood is dark and clotted, bright red blood often appears at the periphery of the clot on the fourth to sixth day. This is the result of early dissolution of the clot and does not necessarily indicate a secondary hemorrhage. Secondary hemorrhage into the anterior chamber results in a markedly worse prognosis. Edwards and Layden17 noted a complication rate of 22% in eyes without secondary hemorrhage but in 58% of eyes that rebled. The secondary bleeding may result in increased IOP and corneal blood staining and is associated with a poorer visual prognosis. Eventual visual recovery to an acuity of 20/50 (6/15) (the metric equivalent is given in parentheses after the Snellen notation) or better occurs in approximately 64% of patients with secondary hemorrhage, as compared with 79.5% of those in whom no rebleeding occurred.10,11,21 Studies have indicated that the incidence of glaucoma following secondary hemorrhage may be as high as 50%. However, improved surgical technique and earlier intervention may improve the final visual outcome.27, 28, 29 Several studies have documented that secondary hemorrhage occurs more frequently in African-American and Hispanic patients. Spoor and colleagues24 observed secondary hemorrhage in 24.2% of African Americans and in only 4.5% of Caucasians. Three other studies have demonstrated greater secondary hemorrhage rates in African-American patients that were highly significant (p <0.05).21, 25, 26, 27, 28, 29 In our recently reported series, 20% (11 of 54) of the controls had a positive test for sickle cell trait (SA hemoglobin), as measured by hemoglobin electrophoresis. Twelve patients in the control group had secondary hemorrhage, 10 (83%) of whom were African American.27 Thus, 32% (10 of 31) of the African-American patients in the control group had secondary hemorrhage, and 40% of them had SA hemoglobin. Other reports have observed a higher incidence of complications and secondary hemorrhage in this population.18, 21, 24, 28, 29, 30 In our previous series, three of eight (37%) such patients with SA hemoglobin had secondary hemorrhage.21 In addition, we have observed patients who presented with microhyphema, normal IOP, and sickle cell trait or disease develop secondary hemorrhage with resultant optic atrophy. One patient, a 12-year-old African-American girl with microhyphema, developed optic atrophy after secondary hemorrhage (Fig. 7). This patient's highest IOP was 28 mm Hg for 24 hours, despite judicious use of antiglaucomatous therapy. Another report cites nine of 14 eyes (64%) of children with sickle cell trait that developed secondary hemorrhage.31 The sickle cell trait-positive group frequently has a significant risk factor for secondary hemorrhage, increased IOP, and permanent visual impairment in children and adults (Table 1). Elevated IOP of 24 mm Hg for greater than 24 hours requires surgical intervention. Other predictive factors are listed in Table 1.21, 32, 33, 34
TABLE 1. Predictive Factors for Secondary Hemorrhage Sickle cell trait or anemia
COMPLICATIONS OF HYPHEMA Four complications of traumatic hyphema, that may be directly attributed to the retention of blood in the anterior chamber, include posterior synechiae, peripheral anterior synechiae, corneal blood staining, and optic atrophy.10,35 Optic atrophy may result from either acute, transiently elevated IOP or chronically elevated IOP. The occurrence of each of these was studied in a series of hyphema patients in an attempt to identify predisposing factors10,32; the results are discussed later. Posterior Synechiae Formation Posterior synechiae may form in patients with traumatic hyphema. This is secondary to iritis or iridocyclitis. However, they are relatively rare complications in patients treated medically. It occurs more frequently in patients who have had surgical evacuation of the hyphema. (It is possible that patients requiring surgery had worse hyphemas and might have developed posterior synechiae even if surgery had not been performed; alternatively, this may be a combined postsurgical-posttraumatic result.) Peripheral Anterior Synechiae Peripheral anterior synechiae occur frequently in medically treated patients in whom the hyphema has remained in the anterior chamber for a prolonged period (9 days or more). The pathogenesis of peripheral anterior synechiae in traumatic hyphema is not definitely established. They may be due to a prolonged iritis associated with the initial trauma and/or chemical iritis resulting from blood in the anterior chamber. Alternately, the clot in the chamber angle may subsequently organize, producing a fibrosis that closes the angle. Both mechanisms may be involved.10,21 Corneal Blood Staining Corneal blood staining occurs primarily in patients who have a total hyphema and associated elevation of IOP (Fig. 8). The following factors may increase the likelihood of corneal blood staining: (1) the initial state of the corneal endothelium (decreased viability resulting from trauma or advanced age (e.g., cornea guttata), (2) surgical trauma to the endothelium, (3) a large amount of formed clot in contact with the endothelium, and (4) prolonged elevation of IOP. All these factors affect endothelial integrity. Corneal blood staining may occur with low or normal IOPs; on rare occasions it may also occur in hyphemas that are less than total. However, these latter two instances can probably be anticipated only in eyes with a severely damaged or compromised endothelium. Corneal blood staining has a greater potential for occurrence in patients who have a total hyphema that remains for at least 6 days with concomitant, continuous IOPs above 25 mm Hg.21 Corneal blood staining may require several months to 2 years to clear.
Optic Atrophy Nonglaucomatous optic atrophy in hyphema patients may be due to the initial trauma or to transient periods of markedly elevated IOP. Diffuse optic pallor (and not glaucomatous cupping) is the result of transient periods of markedly elevated IOP and occurs with constant pressure of 50 mm Hg or higher for 5 days or 35 mm Hg or higher for 7 days.10,21 We have observed a number of patients with sickle cell trait who developed a nonglaucomatous optic atrophy with relatively small elevations of IOP of 35 to 39 mm Hg for 2 to 4 days.21 Despite maximum medical therapy, final visual acuity was less than 20/400 in all patients. We continue to observe optic atrophy in sickle cell trait patients referred to our institution who have not had vigorous control of IOP and/or have had delay in paracentesis. Other studies indicate that patients with sickle cell hemoglobinopathies and anterior chamber hyphemas have more sickled erythrocytes in their anterior chambers than in their circulating venous blood.30 The sickled erythrocytes obstruct the trabecular meshwork more effectively than normal cells, and there is a consequent elevation of IOP to greater levels with lesser amounts of hyphema. Systemic hypotensive agents may not always be successful in reducing the IOP. They may, in fact, be contraindicated in high or repeated dose regimens, because of their possible contribution to intravascular hemoconcentration and increased microvascular sludging, both of which are detrimental in sickle cell hemoglobinopathy. It is possible that the increased IOP is tolerated less well in these patients because of the increased susceptibility to impaired vascular perfusion within the optic nerve and retina. Indeed, moderate elevation of IOP in patients with sickle cell hemoglobinopathy may produce rapid deterioration of visual function resulting from profound reduction of central retinal artery and posterior ciliary artery perfusion.36,37 For these black and Hispanic patients, the prevention of secondary hemorrhage is a critical factor. PROGNOSIS AND TREATMENT The prognosis for visual recovery is directly related to three factors:
Treatment modalities should be directed at reducing the incidence of secondary hemorrhage and reducing the risk of corneal blood staining and optic atrophy. The success of hyphema treatment, as judged by recovery of visual acuity, is good in approximately 75% of patients. Approximately 80% of hyphema patients with less than one-third filling of the anterior chamber regain visual acuity of 20/40 (6/12) or better. Approximately 60% of those with greater than half and less than total hyphema regain 20/40 or better, whereas only approximately 35% of those with an initially total hyphema have good visual results. Approximately 60% of hyphema patients younger than age 6 have good visual results; older age groups have progressively higher percentages of good visual recovery. The severity of the trauma is frequently related to the final visual outcome. Lens opacities, choroidal rupture, vitreous hemorrhage, angle recession glaucoma, and retinal detachment are commonly associated with traumatic hyphema, compromising the final visual result. Fourteen percent of patients have poor visual results from associated trauma, that is, glaucoma, vitreous hemorrhage, retinal detachment, and scleral rupture. Poor visual outcome in traumatic hyphema can be attributed directly to the hyphema in 11% of patients.10,38 This is usually the result of secondary hemorrhage associated with optic atrophy or corneal blood staining. MEDICAL MANAGEMENT The major goals of treatment of traumatic hyphema are to prevent secondary hemorrhage, control IOP, and prevent complications including optic atrophy and corneal blood staining. Generally, medical management seems to produce the best visual result for most patients with less than 75% hyphema.11,21 Surgical intervention is not usually indicated for hyphemas that occupy less than half of the anterior chamber (with the exception of sickle cell patients), because these hyphemas (either primary or secondary) usually resolve spontaneously under medical regiment. In two prospective series totaling 196 patients, neither corneal blood staining nor optic atrophy was noted in hyphemas of 50% or less.10,11,21 Several studies provide evidence that there is no statistically significant difference in most areas of comparison between patients treated by bed rest, bilateral patches, and sedation and those patients treated with ambulation, a patch and shield on the injured eye only, and no sedation.10,11,17 We recommend limited ambulation with bathroom privileges and a patch and shield for the injured eye. Others recommend bed rest, sedation, and patch and shield. We recommend sedation only in the extremely apprehensive or hyperactive pediatric patient. If analgesics are required for the relief of pain, we prefer acetaminophen and/or codeine, depending on the severity of the pain. The antiplatelet effect of aspirin tends to increase the incidence of rebleeding in traumatic hyphema and should be avoided.33 Nonsteroidal anti-inflammatory drugs with analgesic activity, such as mefenamic acid, also share this antiplatelet effect. In any therapeutic regimen, the injured globe requires adequate protection with a patch and shield. Elevating the head of the bed to 30 degrees to 45 degrees facilitates settling of the hyphema in the inferior anterior chamber and aids in classifying the hyphema. Inferior settling facilitates more rapid improvement of visual acuity, earlier evaluation of the posterior pole, and greater clearing of the anterior chamber angle. Also, a better estimate of the decrease or increase in the amount of blood in the anterior chamber is possible during subsequent biomicroscope examinations. Numerous topical medications have been recommended for the treatment of traumatic hyphema, including cycloplegics for the traumatic iridocyclitis and miotics to increase the surface area of the iris to enhance resorption of the hyphema.39, 40, 41 Topical corticosteroids and estrogens have shown contradictory results.41 Definitive evidence of the therapeutic advantages of most topical medications is not available.18,42 Atropine sulfate 1% is indicated for iritis and to break the pupillary block.39 Topical use of steroids after the third or fourth day of retained hyphema may be advantageous to decrease the associated iridocyclitis and prevent or deter the development of peripheral or posterior synechiae. One of our double-masked studies indicates the value of systemic administration of aminocaproic acid (ACA) in the prevention of recurrent hemorrhages.21 If secondary hemorrhages are the result of lysis and retraction of a clot that has produced an occlusion of the traumatized vessel, then prevention of normally occurring clot lysis for 5 or 6 days should be advantageous to allow the injured blood vessel to more completely repair its integrity.21 The antifibrinolytic activity of ACA given systemically has been demonstrated in other areas of the body to decrease the incidence of secondary hemorrhage. ACA retards clot lysis by preventing plasmin from binding to lysine molecules in the fibrin clot. ACA, a lysine analogue, competitively inactivates plasmin by occupying the lysine binding site on plasmin that would normally bind to fibrin. In addition, ACA binds to plasminogen, so that when activated to plasmin, it cannot attach to fibrin. These effects stabilize the clot-vessel wall interface, decreasing the potential for secondary hemorrhage.11,21,27 Based on the work of Ablondi and coworkers43 and Alkjaersig and coworkers,44 a concentration of ACA of 10 to 32.5 μg/ml is required to produce antifibrinolytic effects. These concentrations are achieved in aqueous humor after systemic administration.45 When ACA was administered in a dosage of 100 mg/kg every 4 hours, orally, for 5 full days, a statistically significant reduction in the incidence of rebleeding of traumatic hyphemas was observed.21 Systemic ACA should be used in hyphemas that occupy 75% or less of the anterior chamber because the clot may persist in the anterior chamber for an increased period during administration of the drug. The continued retention of the clot in the anterior chamber would be a disadvantage with larger grade 4 hyphemas. In our prospective study, as well as in two additional studies, patient groups treated with ACA and placebo were randomized and double masked.21,25,46 In the ACA treated group, the incidence of secondary hemorrhage varied between 3% and 4%.21,25,46 In the placebo treated group, the incidence was 28% to 33%. ACA in a dosage of 50 mg/kg every 4 hours is equally as effective as 100 mg/kg every 4 hours, orally, for 5 days.25 The total dosage of ACA should not exceed 30 grams per day. Treatment can be administered on an outpatient basis after 24 or 48 hours if postural hypotension is not observed. Postural hypotension is generally observed in adults but not in children. In many cases, ophthalmologists may chose to initially treat hyphemas with topical medications and carefully monitor the course of blood resolution. However, in selected cases such as those with sickle cell trait or disease, in severe trauma, and in those with rebleeds, ACA can be efficacious. ACA should not be used in pregnant patients or those with renal or hepatic impairment. Because systemic ACA significantly reduces the incidence of secondary hemorrhage, a topical preparation could decrease the incidence of adverse effects. By concentrating the drug in the aqueous humor, a topical preparation would decrease the systemic concentration of ACA associated with many of the adverse effects. Our long-range goal is to improve the treatment of hyphema by decreasing the incidence of secondary hemorrhage using topical drug therapy that is more effective, less toxic, and better accepted by both patients and ophthalmologists than the currently available oral therapy with ACA. For systemically administered ACA to be effective, it must penetrate into the anterior segment in sufficient concentration to retard fibrinolysis. To directly determine the concentration of ACA in aqueous humor following systemic administration, we used an animal model to compare plasma and aqueous humor concentrations of ACA following intravenous (IV) administration of 50 mg/kg and 100 mg/kg, as well as after constant infusion of 25 mg/kg/hr.45 Plasma levels after IV administration were 10-fold higher than in the aqueous humor. Antifibrinolytic activity correlated directly with ACA concentration in plasma or aqueous humor. The time to clot dissolution was greatest (2.5 times control) when the ACA concentration in the aqueous humor reached 30 to 35 mg/dl, which, thus, became our target concentration to achieve with topical therapy. Seven preparations containing ACA were studied to assess which could deliver the required mount of ACA into the aqueous humor.47 The greatest ACA concentrations were obtained using either polyvinyl alcohol or carboxypolymethylene (CPM), 51 and 58 mg/dl, respectively. The latter had a longer duration of action. Using an experimental model for hyphema, ACA in CPM was applied topically every 6 hours for 6 days or until a secondary hemorrhage occurred.48 Compared with no treatment, or the administration of a placebo (e.g., vehicle without ACA), topical application of ACA significantly decreased the incidence of rebleeds from 33% to 10% (p <0.05). There were no ocular side effects after topical application of either formulation. Additional studies have been performed to optimize the concentration of vehicle and drug.49 The optimal combination is 30% ACA to 2% CPM. This combination, however, did not lead to an increase in the duration of action using hyaluronic acid (Healon) or collagen shields as a depot.50 We established a prospective, multicenter, double-masked, randomized clinical trial comparing oral and topical ACA.27 Sixty-four patients with traumatic hyphema treated with topical or systemic ACA were compared with 54 control patients with hyphema. Compared with the control group, topical and systemic ACA were statistically significant in preventing secondary hemorrhage. Only 3% (2/64) of the patients who received topical (35 patients) or systemic (29 patients) ACA had secondary hemorrhage, compared with 22% (12/54) of the control group (p = 0.002). Final visual acuity was 20/40 or better in 30 patients (86%) in the topical group, compared with 23 patients (43%) in the control group (p = 0.001). Final visual acuity was 20/40 or better in 20 patients (69%) in the systemic ACA group, compared with 23 patients (43%) in the control group (p = 0.04). The topical ACA group had a final visual acuity of 20/40 or better in 86% of patients, compared with 69% of patients in the systemic group.27 Topical ACA, thus, appears to be a safe, effective treatment to prevent secondary hemorrhage in traumatic hyphema. It is as effective as systemic ACA in reducing secondary hemorrhage, and no systemic side effects were observed with topical use. Topical ACA provides an effective outpatient treatment for traumatic hyphemas. Although not approved for ophthalmic use in the United States, another lysine analog, tranexamic acid, also has antifibrinolytic properties. In a series of children treated with tranexamic acid, 25 mg/kg/day, the incidence of secondary hemorrhage was significantly reduced.51 The maximum dose is 1500 mg/day for 5 days. Like ACA, tranexamic acid has been associated with nausea, vomiting, and hypotension. Unlike ACA, tranexamic acid is associated with visual abnormalities, which could complicate ophthalmologic evaluation of the patient. In addition, some patients in this study were also treated with other drugs including topical steroids. Other investigators have suggested that systemic steroids decrease the incidence of secondary hemorrhage. Initial studies supporting this claim were not randomized or double masked.40,52 A randomized, double-masked, prospective study by Spoor and associates53 observed a secondary hemorrhage of 20% in controls and 13% in treated patients, not statistically significant. Farber and colleagues54 compared treatment with oral ACA to oral prednisone in a well-controlled trial. Their study suggested that both drugs decrease the incidence of secondary hemorrhage by a similar amount, albeit by different mechanisms. Because of the small number of rebleeds, the confidence limits were large and may have masked a real difference. The major difficulty with this study was that there were no controls. The lack of a true control population is unfortunate in comparing the two groups. In addition, the study excluded all patients with sickle cell trait. These patients are one group that should be considered for systemic ACA or systemic corticosteroid treatment. In addition, patients with gastric ulcer or diabetes mellitus and those that were intoxicated or had bleeding were excluded. The pharmacologic mode of action of the prednisone is unclear and may be related to an anti-inflammatory influence on traumatized blood vessels with reduced engorgement and a propensity for rebleeding. Additional randomized studies with controls to determine whether there is a significant reduction of secondary hemorrhage with systemic prednisone in comparison to systemic ACA would be helpful. Some studies have investigated the application of intracameral tissue plasminogen activator (t-PA) in the management of traumatic hyphema. However, these studies have been neither large nor randomized. A potential problem with t-PA is the associated risk of developing rebleeding of the initial wound. Application of t-PA has been considered in resolving hyphemas that either fail to clear spontaneously or are associated with malignant IOP, although the actual timing of t-PA administration from initial injury has yet to be determined. Topical antiglaucomatous medications usually lower IOP. With the advent of newer glaucoma modalities, we recommend the following: Initiate therapy incrementally with brimonidine tartrate (Alphagan, Irvine CA), followed by latanoprost (Xalatan, Pharmacia Upjohn, Peapack, NJ) and timolol maleate (Timoptic-XE, Merck, West Point, PA). If IOP is still elevated, add a topical carbonic anhydrase inhibitor. In sickle cell trait or disease, methazolamide and topical beta-blockers should be substituted. Miotic agents and sympathomimetic agents are not recommended because of their inflammatory potential. If IOP is still uncontrolled, systemic medication should be given during the acute phase of the hyphema. Acetazolamide, 20 mg/kg/day, may be administered in four divided doses for pressures above 22 mm Hg. However, acetazolamide, can increase the concentration of anterior chamber ascorbate. It lowers the pH of human plasma and exacerbates sickling of erythrocytes. Therefore, methazolamide, 10 mg/kg/day, administered in four divided doses is preferred in pediatric patients with sickle cell trait or sickle cell disease.21,30 Osmotic agents (preferably mannitol) should be considered for pressures above 35 mm Hg. Orally administered glycerol is effective; however, nausea and vomiting are often associated with its administration in patients with elevated IOP. Mannitol is given intravenously, 1.5 g/kg (usually in a 10% solution), over a period of approximately 45 minutes. This may be given two times a day (or every 8 hours in patients with extremely high pressure) in an attempt to keep the IOP below 35 mm Hg. Renal output, blood urea nitrogen, and electrolyte values should be monitored in all patients in whom such therapy is continued for several days. A summary of medical treatment is included in Table 2.
TABLE 2. Medical Management of Hyphema Outpatient Treatment Hyphemas comprising less than one third of the anterior chamber Indications for Hospital Admission Sickle cell trait or anemia
OUTPATIENT VERSUS HOSPITALIZATION With increasing emphasis on cost containment, outpatient management of hyphema has become more popular in recent years. Several studies have demonstrated no significant difference in final visual acuities between patients with smaller hyphemas treated at home and those treated in hospitals.11, 27, 55, 56, 57 Indications for hospital admission are in Table 2. Most patients can be treated on an outpatient basis. Microhyphemas can be treated on an outpatient basis, unless secondary hemorrhage occurs or elevated IOP is uncontrolled. Patients with traumatic hyphema occupying less than one third of the anterior chamber can be treated as outpatients with systemic or topical ACA. If the hyphema occupies more than one third of the anterior chamber, IOP is elevated, or both, hospitalization is recommended. The decision to hospitalize also depends on the cooperation of the patient and family members and the extent of ocular injury. For outpatients, daily ocular examinations should be performed and should include an evaluation of the amount of hyphema and IOP. Daily ophthalmic sketches are helpful in estimating the amount and rate of resolution or rebleeding. Applanation tonometry must be performed at least once daily and twice daily in patients with elevated IOPs. For outpatient or inpatient treatment, daily slit-lamp examination for corneal blood staining and IOP should be performed. Minimal blood staining is often difficult to detect against a background of blood in the anterior chamber. The cornea often assumes a yellowish cast, which is reflected from the yellowish fibrinous coagulum in the anterior chamber. The most typical early sign of corneal blood staining is the presence of tiny yellowish granules that initially appear in the posterior third of the corneal stroma. An additional finding is a lack of definition or a blurred appearance of the ordinarily sharply defined fibrillar structure of the involved corneal stroma. The latter is independent of the yellowish color transmitted to the stroma by the contents of the anterior chamber. We have found this sign to be useful in recognizing the very early stages of corneal blood staining. These biomicroscopic signs of corneal blood staining usually precede gross staining by only 24 to 36 hours. Surgical treatment in this early stage may prevent gross staining, and the cornea may clear in 4 to 6 months. However, once grossly visible staining develops, many months may elapse before clearing is complete. A summary of medical treatment is listed in Table 2. SURGICAL INTERVENTION We believe that most hyphemas, including total hyphemas, should be treated medically for the first 4 days. Spontaneous resolution of the hyphema occurs rapidly during this period, and these cases have the best prognosis. In one series of 20 eyes with total hyphemas, four (20%) cleared sufficiently by day 4 to rule out surgery.58 An additional four eyes resolved spontaneously on medical treatment over a longer period. Generally, with the exception of sickle cell trait or anemia, surgery is seldom indicated for hyphema occupying less than 50% of the anterior chamber. Our indications for surgical intervention are shown in Table 3.11,27,28
TABLE 3. Indications for Surgical Intervention Microscopic corneal blood staining at any time
It is best not to delay surgery if IOP remains elevated at 50 mm Hg or more for 4 days. One study noted optic atrophy in 50% of patients with total hyphemas when surgery was delayed. Corneal blood staining occurred in 43% of patients.59 Patients with sickle-cell hemoglobinopathies, and even those with sickle-cell trait, require surgical intervention if IOP is not controlled within 24 hours.21,27,30 SURGERY FOR HYPHEMA Surgery for hyphema should be cautiously approached. In two series involving 196 patients, surgery was performed in only 14 patients (7.1%).10,11,42 Risks of surgery include damage to corneal endothelium, lens, and/or iris; prolapse of intraocular contents; rebleeding; and increased synechiae formation. With the exception of sickle cell trait patients, no patients in our series required surgery if the hyphema occupied less than 50% of the anterior chamber. Generally, we recommend the type of surgical intervention with which the surgeon is most familiar. Hyphema surgery should be preceded by IV acetazolamide and mannitol, if the IOP is elevated above 35 mm Hg. The operation should be performed under general anesthesia in all patients if medically feasible. The technique that is preferred at this time is evacuation of the hyphema with vitrectomy instrumentation.38,60,61 The initial clear corneal incision is made with a diamond blade. To avoid the iris and lens, the blade is oriented and pushed into the anterior chamber in such a manner that it is parallel to the plane of the iris. A 20-gauge instrument, attached to an infusion line of balanced salt solution plus, is then fitted into the anterior chamber. The balanced salt solution bottle should be 30 to 40 cm above the eye to maintain normal IOP. With the vitrectomy cutting port half open and the infusion line in place, it is possible to irrigate and aspirate free blood from the formed clot. The aspiration mode is initially set at 200 mm Hg vacuum and the cutting speed set at 200 cycles per minute for the procedure. Aspiration mode is increased to 400 mm Hg as needed. Extreme care is required to avoid any iris, lens, or corneal endothelium contact. This operative procedure is used to remove the central portion of the clot. It is not necessary to remove the entire clot in the periphery of the anterior chamber. Careful monitoring for postoperative IOP elevation and peripheral anterior synechiae is essential in these patients. If a secondary hemorrhage occurs during the operative procedure, we recommend tamponade of the bleeding by elevation of the infusion bottle to approximately 70 cm above the eye for several minutes. If the bleeding continues, it is helpful to fill the anterior chamber with sodium hyaluronate after evacuating the clot to tamponade the bleeding site. If bleeding persists, bimanual bipolar diathermy is extremely helpful when the bleeding site is visible.62 At the end of the surgical procedure, the anterior chamber is filled with an air bubble. This will help control any secondary bleeding. The corneal incision is closed with two 10-0 nylon sutures. Vitrectomy instrumention has been successful in lowering IOP. Each eye operated on with this technique has shown an initial decrease in IOP associated with the surgery. Paracentesis causes little surgical trauma and relieves the elevated IOP. Paracentesis is especially beneficial in patients with sickle-cell trait or disease. However, the decrease in IOP may be transient, and there may be no appreciable reduction in the amount of the formed clot. Irrigation by a single- or double-needle technique has the advantage of a small incision. We prefer entry at the 1 o'clock position in the right eye and at the 11 o'clock position in the left eye with a diamond blade. The entry should be made through clear cornea. The irrigating needle should extend just through the corneal endothelium, and a slow push-pull maneuver with the single-needle technique washes out the erythrocytes from the anterior chamber clot, often leaving the fibrin matrix. To reduce the likelihood of rebleeding during the operative procedure, care should be taken not to produce violent alterations in the anterior chamber pressure. If rebleeding does occur, sodium hyaluronate can be effectively introduced for tamponade. After a 5-minute wait, irrigation maneuvers can then be resumed. The one- or two-needle technique has some disadvantages. The surgeon must be particularly careful to have direct visualization of the anterior chamber. Maintaining the position of the needle tip in the anterior chamber may be difficult during the procedure. A hazardous situation is created when the collar-button type of formed clot occupies both the anterior and posterior chambers. This produces pupillary block with anterior displacement of the iris-lens diaphragm. A fourth technique is clot removal with trabeculectomy.11,42,58,63 Generally, trabeculectomy is not used in smaller hyphemas. Trabeculectomy with anterior chamber washout and peripheral iridectomy is a beneficial primary surgical treatment for traumatic hyphema unresponsive to medical management with antiglaucomatous agents. Trabeculectomy provides a means to keep IOP lowered while the remaining blood is cleared from the anterior chamber. In patients with total hyphema, trabeculectomy with peripheral iridectomy should strongly be considered. Trabeculectomy is performed with gentle irrigation of the anterior chamber hyphema. Relatively safe, it should be performed early for cases of total hyphema unless the elevated IOP is controlled medically and resolution of the hyphema is clearly imminent. We use this technique in patients with total hyphema at day 4 and find this superior to clot evacuation. Several patients referred to our institution have had attempts at clot evacuation. One patient sustained complete iridodialysis related to attempted clot evacuation. In addition, we have had other patients who have been referred after optic atrophy developed with total hyphemas. When the trabeculectomy surgery is performed, we use a 3 × 3 mm scleral trap door, hinged at the limbus. Superficial episcleral vessels are coagulated with the bipolar cautery. A superficial lamellar flap is developed through one-third scleral thickness creating the trap door hinged at the limbal area. Peripheral iridectomy is performed followed by gentle irrigation of the clot in the area of the trabeculectomy site. Two 10-0 nylon sutures are used to close the trabeculectomy site. The conjunctiva is closed with a running 7-0 or 8-0 Vicryl suture. Once conjunctiva has healed, the nylon suture(s) can be lasered to open up the trabeculectomy site when necessary. This technique has been invaluable in difficult total hyphema cases. Each of these surgical procedures has a set of complications. The surgeon should thus approach each patient with caution and individualize the surgical approach. SUMMARY Traumatic hyphema continues to be one of the challenging clinical entities encountered by the ophthalmologist. Even a small hyphema can be a sign of a major intraocular trauma with associated damage to other intraocular tissues. The potential for secondary hemorrhage and the secondary onset of glaucoma may transform an eye with an initially good visual prognosis into one with a poor visual prognosis. IOP is the most important parameter for therapeutic decision making with traumatic hyphema. Even small accumulations of blood in the anterior chamber can be a concern with elevated pressure in patients with sickle cell trait or disease. These patients may develop sickling in the anterior chamber and elevated pressure, and problems may result with retinal circulation causing vascular occlusion. Treatment modalities should be directed at controlling the IOP, reducing the incidence of secondary hemorrhage, and reducing the associated visual complications of corneal blood staining and optic atrophy. It used to be common practice to hospitalize all hyphema patients; however, now many patients with smaller hyphemas are treated on an outpatient basis. For hyphemas occupying more than one third of the anterior chamber, hospitalization during the first 5 days of treatment after injury (the period of greatest risk for rebleeding) remains justifiable and is one way to ensure daily biomicroscopy. The prognosis for visual recovery in traumatic hyphema is directly related to three factors: (1) the amount of associated damage done to ocular structures (e.g., choroidal rupture or commotio retina with associated macular scarring); (2) the occurrence of secondary hemorrhage; and (3) the occurrence of complications of glaucoma, corneal blood staining, and optic atrophy. |
| TRAUMA TO THE SCLERA | |||
RUPTURE AND LACERATIONS Ocular findings associated with scleral rupture include marked chemosis, hyphema (frequently total), a deeper-than-normal anterior chamber, below normal or very low intraocular tensions, and reduced ductions (usually more pronounced in the quadrant of scleral rupture).64 The large hyphema often precludes initial estimation of the anterior chamber depth and ophthalmoscopic examination. Blow-out fractures may coexist but are rarely associated with scleral ruptures. A diagnosis of scleral rupture should not be excluded solely on the basis of normal or even increased ocular tensions. Although ocular tensions are frequently below 4 mm Hg, the scleral defect may be sufficiently closed by blood clot or orbital tissue to allow the IOP to rise. In the presence of a normal ocular tension, a thorough examination is still warranted. Blunt scleral ruptures frequently occur at or near the limbus. Others occur posterior to the rectus insertions where the sclera is thin.64 Most scleral ruptures are found anterior to the equator, but approximately 10% to 20% are located posterior to the equator. Marked conjunctival hemorrhage or chemosis often indicates scleral rupture, especially when either sign is disproportionate to other indications of injury (Fig. 9). Conjunctival chemosis is usually generalized, but it may be confined to one or two quadrants in scleral rupture. Other signs include markedly reduced visual acuity, shallow anterior chamber, hyphema, pupillary distortion, and subconjunctival coloring from prolapsed uveal tissue.65
Scleral ruptures may be divided into two types: direct (i.e., those occurring immediately at the site of mechanical impact) and indirect (i.e., those occurring at a scleral site remote from the site of trauma). In most instances the rupture is occult, that is, it is covered with conjunctiva and is not immediately visible on external examination. The left eye is more frequently involved than the right, because most assailants are right handed and tend to strike the victim's more vulnerable inferotemporal aspect of the left eye. The most frequent sites of scleral rupture are (1) at the limbus, (2) parallel to the equator (between the rectus muscle insertions and the equator), and (3) perpendicular to the limbus (usually under the rectus muscles). (see Fig. 8) Less frequent sites are in the cornea and at the posterior pole. Limbal ruptures are most frequently found opposite the site of impact (in the superior nasal quadrant). Posterior ruptures, lying parallel to the equator, are more often found superiorly in either the nasal or the temporal quadrant.3 Posterior scleral ruptures can be the result of double perforating projectiles. Differentiation may be difficult between a rupture by blunt trauma and laceration delivered with considerable force by a semisharp object, because the signs of trauma are prominent in each of these injuries. In contrast, the signs of trauma produced by sharp objects may be subtle and mild. In combined corneoscleral lacerations, the anterior chamber is often flat or shallow, and the uveal tissue may be prolapsed through the wound or incarcerated in it.3 Hyphema and vitreous hemorrhage frequently occur; also, there often is external bleeding from the injured sclera. Scleral lacerations are sometimes occult, like scleral ruptures. When caused by a thin, penetrating object, the laceration may be extremely subtle. Scleral laceration should be suspected with any conjunctival laceration and with lacerations of the upper or lower lids, even as far as the orbital rims. A minute laceration of the eyebrow induced by a scissors point has been known to produce a superior equatorial laceration that would have gone unrecognized without a meticulous ocular examination.66 OPERATIVE REPAIR While awaiting surgical repair, the lacerated or ruptured eye should be protected by a patch and shield. Blepharospasm may be relieved with an analgesic or, in unusually severe cases, with a facial nerve block. With a suspected open globe, lid sutures instead of a speculum should be used. Any material wiped from the lids during the initial examination should be carefully examined for intraocular contents and, if necessary, submitted to the laboratory for pathologic examination. For contaminated wound, tetanus immunization and parenteral administration of broad-spectrum antibiotics should be instituted early in the course of therapy. We recommend a 360-degree peritomy and scleral exploration whenever there is the slightest suggestion of scleral rupture or laceration. Scleral exploration produces few, if any, postoperative complications and provides valuable information. Early discovery of the scleral defect may help minimize herniation of intraocular contents, produce a primary repair, and prevent fibrous ingrowth. Scleral repair is usually accomplished by closure of the sclera with interrupted sutures. The initial sutures in corneoscleral lacerations should be placed at the limbus for best apposition. The limbal sutures restore correct anatomic relationships. We prefer 8-0 or 9-0 nylon sutures. Any prolapsed iris should be repositioned. Normal globe contours must be re-established. If there is a large scleral defect, a graft of preserved sclera will help to bridge and close the wound.67 One should not excise scleral tissue unless sufficient donor material is available. Defects located posterior to the ora serrata should be treated around the site of rupture or laceration with diathermy or cryotherapy in an attempt to prevent spreading or retinal detachment. The ora serrata may be precisely located by transillumination of the globe through the pupil; this outlines the dark shadow of the ciliary body. Buckling the scleral repair with a sponge-type exoplant also may be useful, if excessive vitreous traction is anticipated. Uveal prolapse from a scleral laceration should be reposited. There is a risk of excising retinal tissue if the laceration is posterior to the pars plana. The best method is closing scleral tissue with prolapsed uvea is to close the wound initially at the anterior or limbal area and then proceed posteriorly with closure with interrupted sutures. It is best to pass the suture needle completely through one end of the sclera before a second pass. If the uvea does not reposit readily, a cyclodialysis spatula can depress the prolapsed uvea as the sclera is closed. Posterior vitreous prolapse and incarceration usually mean severe retinal damage is present. Indications and techniques regarding vitrectomy with scleral lacerations are discussed elsewhere in Clinical Ophthalmology. Generally, vitrectomy is indicated with scleral lacerations if significant vitreous hemorrhage or nonmagnetic foreign body or cataract is noted at the time of injury.67 Ruptures at the limbus and anterior to the pars plana should be repaired similarly; however, diathermy and cryotherapy are not required. A more cosmetically acceptable repair is created with 6-0 Mersilene or 9-0 nylon sutures than with stouter material. Fine suture material such as 10-0 nylon may be used if the repair continues into the sclera from a laceration that is primarily corneal. Following wound closure, prophylactic intravitreal injections may include broad-spectrum antibiotics and steroids, although some controversy still persists regarding specific protocols. The prognosis for good recovery of vision is poor with major ocular injuries. (see Fig. 4 and Figs. 10 and 11) However, the potential for return of useful vision justifies an attempt at repair whenever feasible. Enucleation at the time of the original surgical procedure (primary enucleation) should be considered only in the event of total disruption of the globe; this includes those patients in whom large amounts of intraocular contents have been extruded or who have large scleral lacerations or ruptures that are completely irreparable. Initial repair permits evaluation of the total ocular status in the immediate postoperative period, with possible secondary enucleation at a later date. Thus, the patient is allowed a period of mental recovery to a more alert and oriented state. Also, the patient recognizes that the surgeon is making all possible efforts to salvage the injured globe.
Enucleation should be considered in the early postoperative period (within approximately 1 week after injury): (1) when the eye no longer has light perception, (2) when projection of light becomes inaccurate, or (3) when the visual prognosis is hopeless. With these as the criteria for enucleation, the incidence of sympathetic ophthalmia has been significantly minimized. |
| TRAUMA TO THE CHOROID | ||||||||
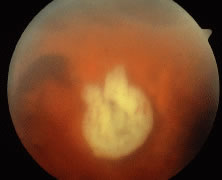
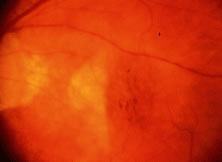
Blunt trauma may produce hemorrhage
into the choroid. When blunt trauma results in globe anteroposterior compression,
the relatively inelastic Bruch's membrane is prone to rupture and the overlying
retinal pigment epithelium and underlying choriocapillaries tend to tear.
The picture on fundus examination is a choroidal rupture (Figs.
12, 13, and 14).
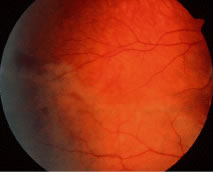
Generally, direct ruptures are anterior and oriented parallel to the ora.
Direct choroidal ruptures are relatively rare and are the result of compression
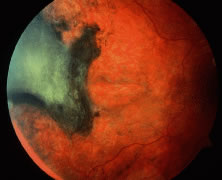
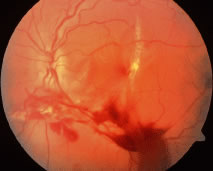
necrosis. Indirect choroidal ruptures are away from the site of impact and
tend to be crescent shaped and posterior. Frequently, the rupture is concentric
to the optic nerve and adjacent to the macular area (Figs.
15 and 16). This may involve
a small peripheral area, or it may be massive and break through Bruch's
membrane to produce additional subretinal, retinal, subhyaloid, and/or vitreous
hemorrhage (Figs. 17 and 18).
The typical small choroidal hemorrhage is a rounded, dark red-blue mound
with pinkish edges, located most frequently at the equator or adjacent to
the disc. These areas frequently take many weeks to resorb and may leave
areas of pigmentary alteration. A potential complication of choroidal rupture
is chorioretinal vascular anastomosis as described by Goldberg.68
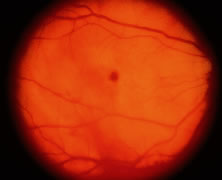
Blunt trauma commonly produces retinal edema. Berlin's edema or commotio retinae can affect the entire posterior pole (Fig. 19). Visual acuity may be reduced and late pigmentary changes may occur in the posterior pole, especially in the macular area.3
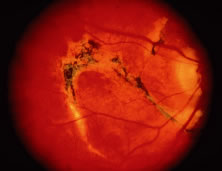
Massive subchoroidal hemorrhage may cause detachment of a large area of the choroid. This is often associated with profound secondary glaucoma, as well as extensive destruction, and it does not usually respond to therapy. If the condition is recognized early enough, sclerotomy may be attempted in the same fashion as when dealing with an expulsive hemorrhage during intraocular surgery. Lesser choroidal detachments are frequently found in the temporal aspect of the injured globe. The treatment is cycloplegia and close observation. Choroidal tears frequently follow severe ocular contusion. When this injury occurs in the posterior pole, it appears to result from a contrecoup mechanism. Choroidal, retinal, and vitreous hemorrhages are frequently associated with the choroidal tear, obscuring the choroidal injury during the early posttraumatic period. With resorption of the hemorrhage, a yellow-white crescent-like scar appears. This is often vertical, temporal to the disc, and concentric to it. The scar is usually single; however, there may be multiple scars parallel to each other. The sclera is seen through the defect, and retinal vessels and the retina are often intact over it. Permanent visual impairment occurs in the immediate area, especially when the macula is involved. Nerve fiber bundle defects may occasionally result when the injury is adjacent to the disc and the overlying retina is involved. |