|
|

|
| Chapter 9A Giant Papillary Conjunctivitis E. LEE STOCK and DAVID M. MEISLER Table Of Contents |
|
PATHOPHYSIOLOGY PATHOLOGY TREATMENT REFERENCES |
Giant papillary conjunctivitis (GPC), first described by Spring1 in 1974, is an inflammatory disorder of the external eye. It is most commonly
associated with contact lens wear. It has also been associated
with ocular prostheses2 and exposed sutures. Clinically, GPC is characterized by papillary hypertrophy
of the upper tarsal conjunctiva, similar in appearance to the
papillae seen in vernal conjunctivitis. Itching and burning, discomfort (foreign-body
sensation), and increased mucus production are the symptoms
of GPC.3 Patients usually report a past ocular history of contact lens wear or
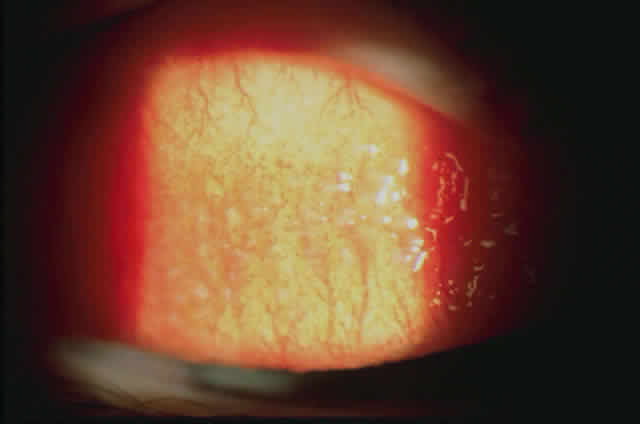
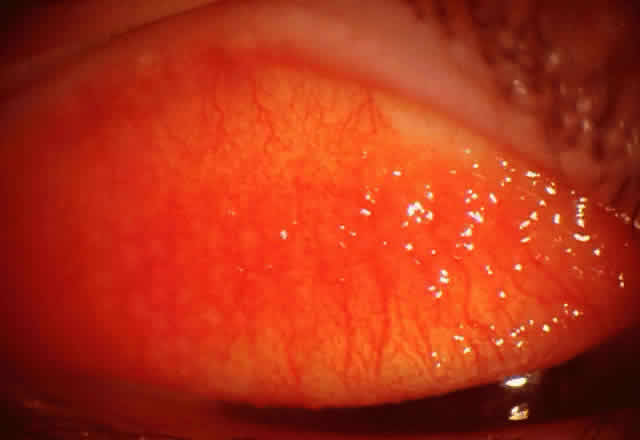
ocular surgery (cataract, keratoplasty, enucleation). The signs of GPC
include mucous discharge, papillary conjunctivitis consisting of enlarged
papillae (Fig. 1), lid swelling, and ptosis and pannus (Fig. 2). Allansmith4 defined giant papillae as those larger than 1 mm. GPC shares other signs
with vernal conjunctivitis, including Trantas' dots and limbal gelatinous
elevations.5 Apical fibrotic-appearing changes of the papillae have been reported clinically, but
it is unclear if these changes are transitory or permanent (Fig. 3).
|
| PATHOPHYSIOLOGY |
| Theories involving immune and mechanical mechanisms have been espoused
in the pathophysiology of GPC. Most theories suggest that proteinaceous
material must be deposited on the lens surface for either the allergic
or the mechanical mechanisms to take effect. ADSORPTION ONTO CONTACT LENSES Deposits on Lenses The adsorption of tear proteins onto the surface of hydrophilic contact lenses6 has been documented by many different methods. The deposits found on spoiled contact lenses include lipids that do not appear to be antigenic,7 and proteins. Many tear proteins that have been identified on contact lenses include lysozyme, lactoferrin, protein G, prealbumin, albumin, and immunoglobulins.8–15 All hydrogel lenses develop a proteinaceous coating that begins almost immediately after insertion.16–18 In a model of protein deposition, a dual layer forms over the contact lens surface immediately after insertion. The first (primary) layer that forms is composed mainly of irreversibly bound denatured proteins. The pellicle, a mucoprotein layer, is partially reversible, is denatured, and tries to equilibrate with the tear film. Lens biocompatibility is largely determined by the primary layer and its biochemical structure because the primary layer is more apt to undergo conformational changes than the second layer. It has been suggested, but not proved, that it is this protein and tear film interaction that ultimately determines whether a contact lens surface is biocompatible. If it is not biocompatible, adverse external ocular responses such as GPC may result.15,19 The type of contact lens may explain how deposits collect on the contact lens surface of patients who develop GPC. The extent to which protein is deposited on the anterior contact lens surface seems to depend on the polymer content, structure, and charge.20,21 Lenses with higher water content tend to develop more deposits than lenses with lower water content.22 The high porosity may allow more tear film components to enter and embed in the contact lens matrix.14,19,23 The net ionic charge of the polymer also influences protein buildup. Lysozyme, a positively charged protein, is attracted to negatively charged ionic materials.24–26 Studies have shown that lenses with both high water content and ionic properties have the greatest deposition of proteinaceous material.6,18,22,27 Furthermore, protein may not deposit uniformly on hydrogels. Some lenses tend to build up protein on the edge, compared with a more uniform distribution on lenses from other groups.28 The hydrogel fabrication process appears to induce a different protein adsorption behavior.29 Lathe-cut lenses tend to adsorb twice the amount of protein as spincast lenses.30 Another study showed lathed hydrogels to have deposits in the lathe marks even after vigorous cleaning.31 It may seem logical to assume that the greater the amount of deposit, the greater the likelihood of developing GPC. However, there has not been a definitive association between GPC with a particular lens type and the amount of protein deposited on the contact lens surface,32 further questioning the importance of proteins. Increased deposition of protein on lenses of some GPC patients may be the result of the inflammatory reaction rather than the cause of the reaction.9,19 Furthermore, the deposits on soft contact lenses of patients with GPC appear no different on scanning electron microscopy from deposits on lenses of asymptomatic wearers.19 BIOCHEMICAL NATURE OF PROTEIN DEPOSITS. The biochemical nature of protein deposits rather than the quantity or appearance of bound protein may be important. For example, once lysozyme is bound irreversibly to the lens surface, it undergoes molecular conformational changes.30,33 Lens-bound protein may be denatured by shearing forces and stresses interacting at the anterior lens surface, such as cyclical drying and rewetting.23 Once lysozyme has been denatured, its interactions with other layers in the tear film are altered and this interaction may play a role in inducing GPC. ALLERGIC HYPOTHESIS Evidence for the allergic theory of GPC includes many studies on the immune reaction in these patients. Most studies have been aimed at immediate hypersensitivity mechanisms. A biopsy study of tissue obtained from a patient with GPC associated with an ocular prosthesis34 found conjunctival plasma cells mostly containing IgE antibody, and to a lesser extent IgG, IgA, and IgM antibody. Another study evaluated tears of 18 patients with GPC and noted the highest level of IgE antibody in the tears of patients with GPC, compared with the IgE tear levels in vernal keratoconjunctivitis. Using transferrin as a marker, these investigators confirmed the suggestion that the IgE antibody was locally produced.35 Contact lens deposits expected to mediate an immunologic response in GPC have also been investigated. Refojo and Holly36 in 1977 suggested that tear protein adsorbed onto the contact lens surface might produce contact lens allergy. Strong anecdotal support for this notion includes the finding of accumulated surface deposits on contact lenses from GPC patients.37 Replacing a worn lens with a new or different lens or cleaning a worn lens often may improve GPC signs and symptoms.38 Asymmetric and unilateral GPC has been observed in the eye wearing the older, dirtier lens.39 In an animal model for GPC, eyes that wore lenses from GPC patients were more likely to develop an inflammatory response akin to GPC than were eyes exposed to unworn soft contact lenses and lenses from asymptomatic wearers.40 An increase in the IgG to IgA deposition ratio has been found on lenses obtained from patients with GPC compared with lenses obtained from asymptomatic contact lens wearers.41 A subsequent study found increased IgM deposition on GPC-associated contact lenses42 but could not confirm the increased IgG to IgA ratio. Eosinophil major basic protein is material elaborated from eosinophils attracted to allergic reactions. This material was not deposited to a significant degree on contact lenses obtained from GPC patients.43,43a MECHANICAL HYPOTHESIS In contrast, and in support of the mechanical theory, investigators have been unable to confirm a direct immunologic role of the contact lens. One animal study suggested that the polymeric composition of one soft contact lens material was not particularly antigenic and therefore unlikely to incite GPC via an immunologic reaction.44 Hypersensitivity testing of contact lens-intolerant patients with contact lens material has revealed infrequent reactivity.45,46 The mechanically induced hypothesis has been supported by the association between GPC and inert objects such as exposed sutures, extruded scleral buckles, cyanoacrylate adhesives, and a keratinized limbal dermoid cyst.4,46a The fact that GPC has produced bloody tears presumably due to conjunctival irritation and friction gives further support to the mechanical theory. Neutrophil chemotactic factors (NCF) thought to originate from damaged conjunctival epithelial cells have been found in the tears of symptomatic GPC patients at 15 times the level of asymptomatic patients.43 In addition, after injection of these factors into the upper tarsal conjunctiva of rabbits for 7 days, a GPC-like inflammatory reaction was observed. It has been suggested that damage necessary to release NCF may come from a continued assault on the tarsal conjunctiva by the contact lens.43,47 As a result, these findings have led to the theory of a combined pathogenesis for GPC involving both mechanical trauma to the upper tarsal conjunctiva and a hypersensitivity reaction to lens-bound antigens.47,48 |
| PATHOLOGY |
| The epithelium shows a reduction in the number of goblet cells and infiltration with mast cells. Other inflammatory cells, including eosinophils, basophils, and lymphocytes, have also been observed. The stroma has an increased number of inflammatory cells, including lymphocytes and plasma cells, eosinophils and basophils, and degranulating mast cells. In the advanced stages there is proliferation of fibroblasts and deposition of collagen.4 |
| TREATMENT |
REMOVAL OF OFFENDING AGENTS Contact lens wear should be stopped, exposed sutures removed, and adhesive covered or removed. MEDICAL TREATMENT Drugs that stabilize the mast cell and prevent degranulation have been used to treat GPC. Sodium cromolyn drops have been shown to be effective for the treatment of GPC.49 Alomide, a new mast cell stabilizer effective against vernal conjunctivitis, Acular, a prostaglandin inhibitor effective against allergic conjunctivitis, and Levostin, a new antihistamine, have yet to be tested against GPC. Specific types of corticosteroids have been developed to maximize potency and decrease side effects. One of these drugs, loteprednol etabonate, is effective in GPC.50 However, this was a short-term study, and the side effects with prolonged use have not been established. The long-term use of corticosteroids is discouraged in the treatment of GPC because of the potential side effects. Treatment Directed at the Contact Lenses Cleaning contact lenses, replacing a worn lens with a new one, or switching to a different type of contact lens has given relief from GPC. Fitting disposable contact lenses has successfully allowed continued contact lens wear in some GPC patients. However, GPC has been associated with disposable contact lens wear.48 Disposables are not exempt from protein deposition.47,51 Their advantage over conventional hydrogels in the context of GPC is probably not due to the characteristics of the lenses themselves, but possibly the frequency of replacement that may minimize mechanically induced conjunctival trauma and contact lens deposits. Rigid gas-permeable (RGP) contact lenses were and still are used as alternative lenses in the therapeutic strategy for GPC. RGP lenses are smaller than soft lenses and thus present a smaller surface area to the conjunctiva. The edge of a gaspermeable lens can be shaped and reshaped to minimize trauma to the conjunctiva. Finally, deposits are removed more easily from hard lenses than from hydrogel lenses.52 However, GPC occurring in wearers of rigid gas-permeable lenses has been reported.53,54 A retrospective study showed an inverse relationship between DK value and the interval of time between RGP contact lens wear and the onset of GPC.54 It was reasoned that higher DK material with poorer wettability over time was apt to collect deposits, with resultant GPC. The wettability of RGPs has since been enhanced with the creation of fluorinated RGP contact lenses. The difficulty in ascertaining the impact of contact lens type and material on the development of GPC is further hampered by many other variables that may play a role in the pathogenesis of this disorder. They include disinfection methods, cleaning routines, lens thickness, tear pH, blinking mechanisms, lens wettability, and elasticity.19 It is also difficult to control for the effect the external milieu has on the lens/tear interaction in conditions such as blepharitis55,56 and atopic disease.55,57 Other extrinsic factors that may contribute to lens spoilage and GPC include airborne antigens and microbes that adhere to the lens deposits or lens surface. Supported in part by a Department of Veterans Affairs Research Service Grant (ELS). |