|
|
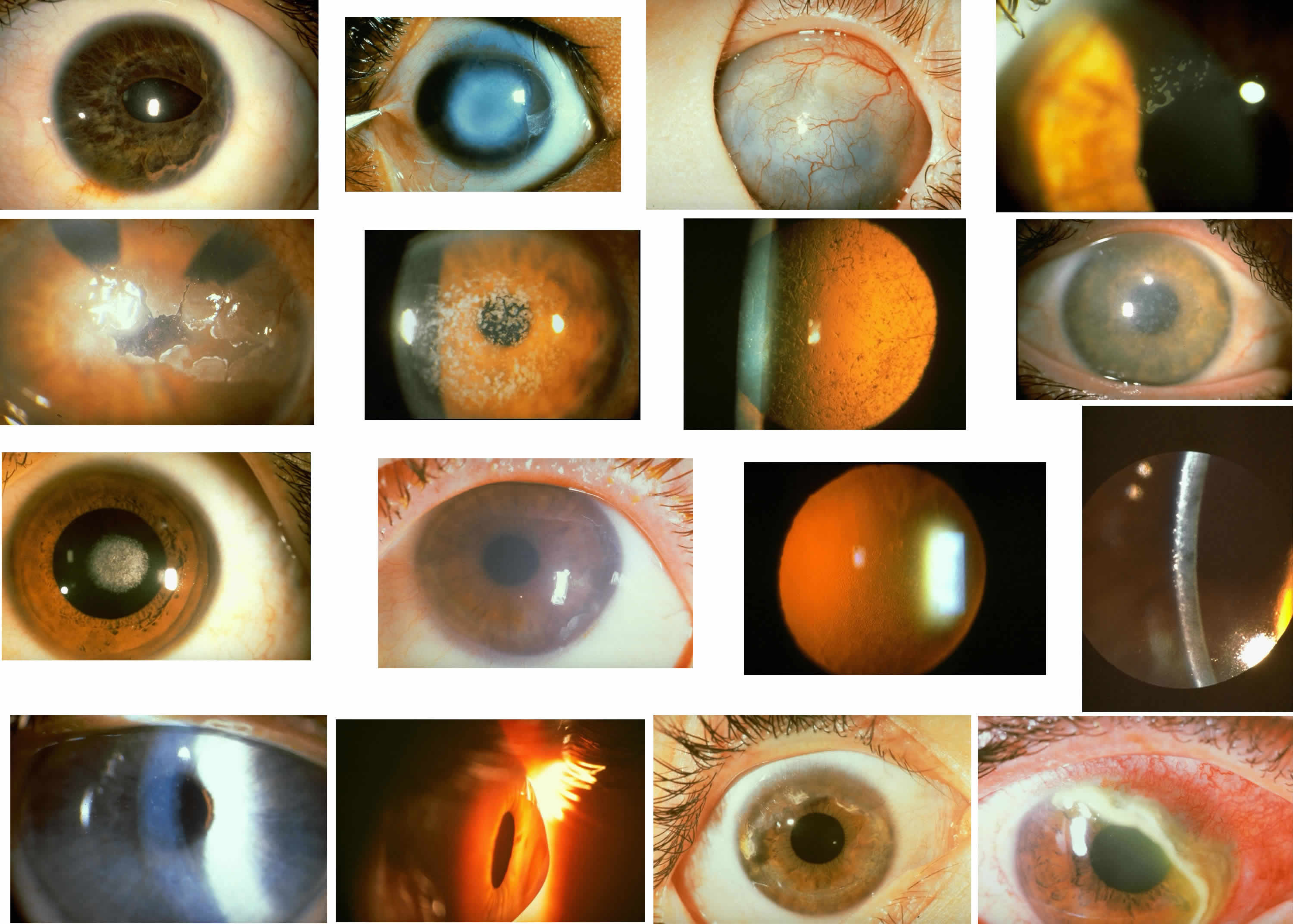
| Color Plate 1 A. Rieger's anomaly. The central cornea is unaffected and visual acuity remains normal. However, there is anterior displacement of Schwalbe's line and broad iridocorneal synechiae with distortion and displacement of the pupil. B. Peters' anomaly. The corneal leukoma is central, corresponding to the defect in Descemet's membrane and endothelium with overlying stromal disorganization. The peripheral cornea remains clear. Not evident are characteristic adhesions between the iris margin and the periphery of the stromal opacity. C. Congenital anterior staphyloma. Extreme stromal ectasia, scarring, and disorganization plus neovascularization are accompanied by congenital glaucoma with anterior buphthalmos. The posterior segment remains relatively unaffected. D. Epithelial basement membrane dystrophy, This variant of map-dot-fingerprint dystrophy displays predominantly small, opaque debris-filled intraepithelial pseudo-cysts, with predisposition to recurrent erosive symptoms. E. Band keratopathy. In this patient with long-standing chronic inflammation subsequent to multiple surgical procedures, extensive calcific deposition at the level of Bowman's layer results in epithelial distortion and erosion. F. Granular corneal dystrophy. This autosomal dominant dystrophy displays discrete stromal opacities with the appearance of snow-flakes or bread crumbs, and since the intervening stroma is clear, visual acuity is maintained. G. Lattice corneal dystrophy. This autosomal dominantly inherited disorder of amyloid metabolism is evident as pathognomonic branching opacities within the corneal stroma, as well as more diffuse subepithelial deposits, best appreciated by retroillumination. H. Macular corneal dystrophy. This autosomal recessive dystrophy displays diffuse full-thickness stromal haze with superimposed focal stromal opacities, affecting both stroma and Descemet's membrane. Since vision is compromised, penetrating keratoplasty is required. I. Central crystalline dystrophy (Schnyder). Fine, needlelike intrastromal crystals, predominantly of cholesterol, are slowly progressive and may be accompanied by arcus. The dystrophy is dominantly inherited and may have concomitant systemic abnormalities of lipid metabolism. J. Congenital hereditary endothelial dystrophy. Diffuse edema of the corneal stroma is accompanied by relatively limited and usually nonprogressive epithelial edema. Thus, visual acuity may be relatively well preserved. K. Fuchs' endothelial dystrophy. The earliest manifestations are evident as myriad focal guttate excrescences of Descemet's membrane in the absence of epithelial or stromal edema. These are best appreciated by retroillumination, and specular microscopy is confirmatory (see also Fig. 17). L. Fuchs' endothelial dystrophy. With a more advanced stage of corneal endothelial dysfunction, stromal and epithelial edema progress with loss of vision and possibly painful bullous epithelial erosion. M. Posterior polymorphous dystrophy. In this moderately advanced case, grouped vesicular opacities at the level of Descemet's membrane probably correspond to fibrous proliferations in the geographic areas of endotheliallike transformation. There is some extent of stromal edema, but visual acuity is usually preserved. N. Keratoconus. The corneal thinning and ectasia result in extensive visual distortion due to irregular astigmatism. O. Terrien's marginal degeneration. In this young man with progressive myopic astigmatism, noninflammatory corneal thinning is evident in the superior periphery. Noteworthy slit lamp findings include neovascularization of the thinned stroma with lipid extravasation at the leading edge without epithelial defect. P. Mooren's ulcer. This inflammatory condition of peripheral ulcerative keratitis is hall-marked by pain in the setting of intense conjunctival inflammation. The overlying peripheral corneal epithelium is ulcerated, as is the corresponding stroma. A dense infiltrate of acute inflammatory cells precedes the active front of progressive ulceration. This case was remarkably improved by simple resection of the adjacent peripheral limbal conjunctiva. |