|
|
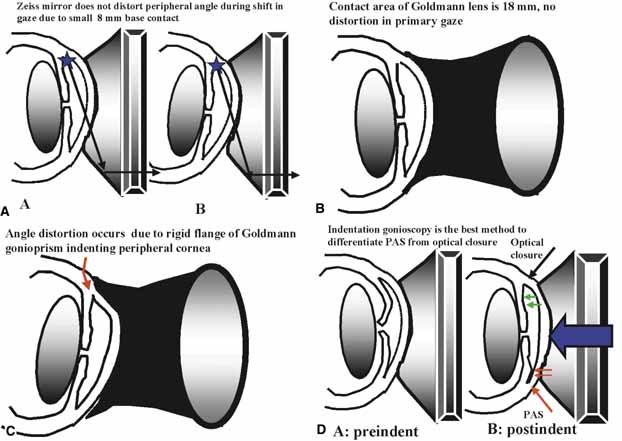
| Fig. 13 Gonioscopic techniques for the narrow-angled eye. A. The small contact area of the Zeiss lens facilitates evaluation of the narrow angled eye. When the last roll of the iris obstructs the view into the recess, have the patient look into the mirror of regard. This helps to bring the angle recess into view. In this figure the examiner is evaluating the superior angle through the inferior mirror. In order to see further into the recess, the patient is instructed to look down, into the mirror of regard. B. The Goldmann lens has a much larger contact area and the edge of the lens compresses the limbus. C. When the patient looks down, the superior flange of the lens compresses the superior limbal area, distorting the peripheral angle. This will artificially narrow the angle and the view is compromised due to striae in the cornea. D. Indentation gonioscopy is an excellent technique to differentiate PAS from optical closure. Indentation gonioscopy is best performed with a Zeiss-type lens. When the examiner is unable to see into the angle recess because of bowing of the iris, compression gonioscopy is essential. With constant pressure, the examiner indents the cornea with enough force to displace aqueous posteriorly into the iris. In areas where the iris is unsupported, the iris separates from the cornea and the angle opens and the recess is seen. If the displaced iris opens all the way in to the recess, it is optical closure and the angle is still likely functional. If the angle opens up only into the meshwork, peripheral anterior synechiae (PAS) are present. In this example, the superior angle is optically closed and the inferior angle is permanently closed. (Figure continues.) |