|
|
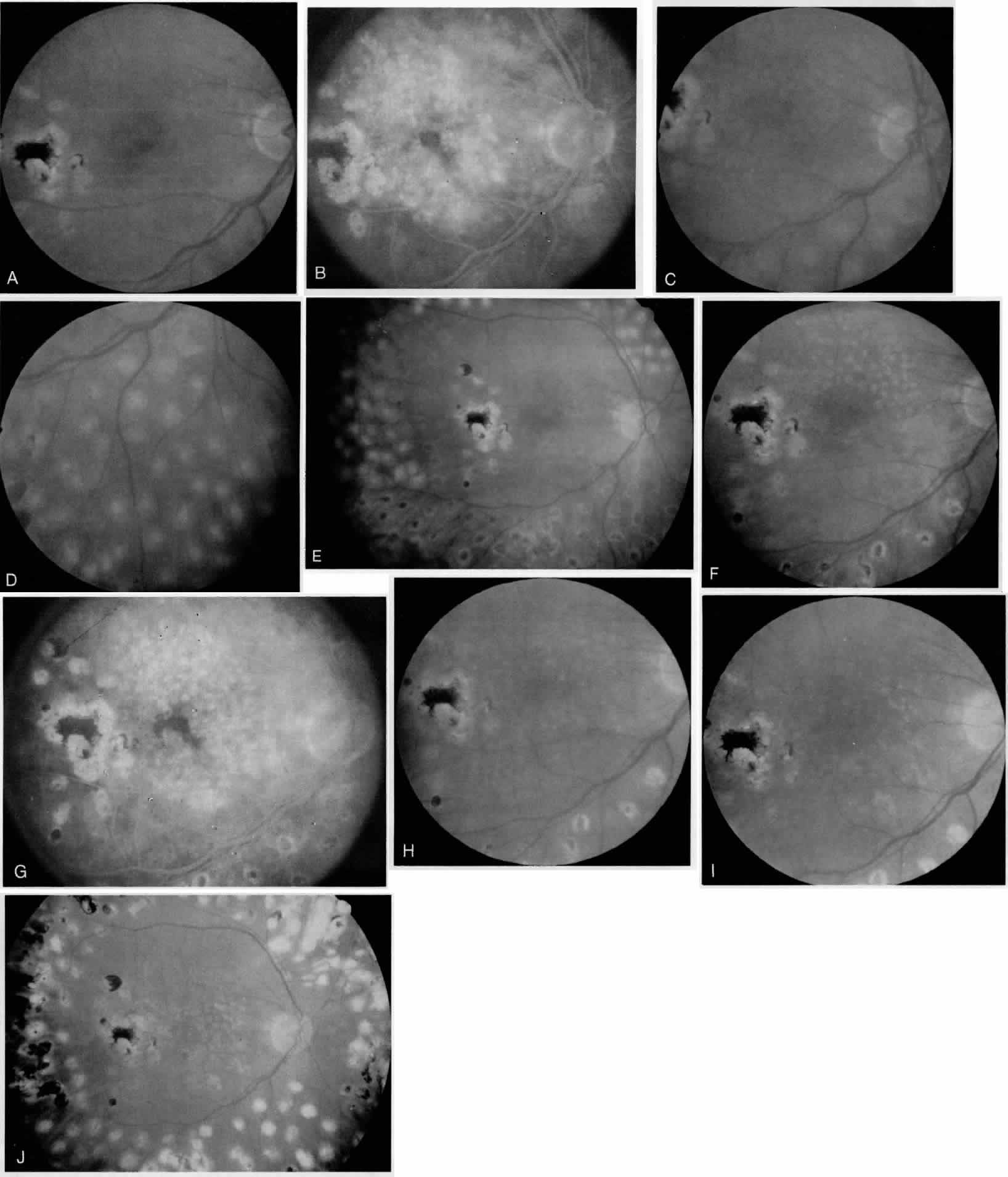
| Fig. 5. Case 5 is a 41-year-old man with a 16-year history of insulin-dependent diabetes who complained of recent decrease in vision in the right eye. He receives previous focal laser photocoagulation for macular edema 5 years prior to presentation; his visual acuity was 20/40. On clinical examination diffuse diabetic macular edema with cystoid macular edema involvong the FAZ and proliferative diabetic retinopathy with NVE and preretinal hemorrhage were noted (A; Color Fig. 5.). Combined treatment of the macular edema and proliferative disease was recommended and fluorescein angiography was performed (B). Modified grid laser photocoagultion combined with panretinal photocoagultion to the interior half of the retina was performed (C, D), followed 2 weeks later with treatment of the superior half of the retina with panretianl photocoagultion (E). Three months later onvolution of the neovascularization and absorbtion of the hemorrhage were seen; however, persistent central macular edema was noted on clinical examination (F). Therefore, fluorescein angiography was performed (G), and supplemental grid laser photocoagultion was given (H). Four months later no residual retinal thickening was observed on clical examination (I). On further follow-up 1 year later, visual acuit remained 20/40 without recurrence of either proliferative or macular disease (J). Comment: Here is a case in which fluorescein angiography is needed for the treatment of diffuse macular edema present in combination with proliferative diabetic retinopathy. The Fluorescein angiogram was obtained because the macular thickening required treatment, and not to determine the need for panretinal photocoagulation. |