|
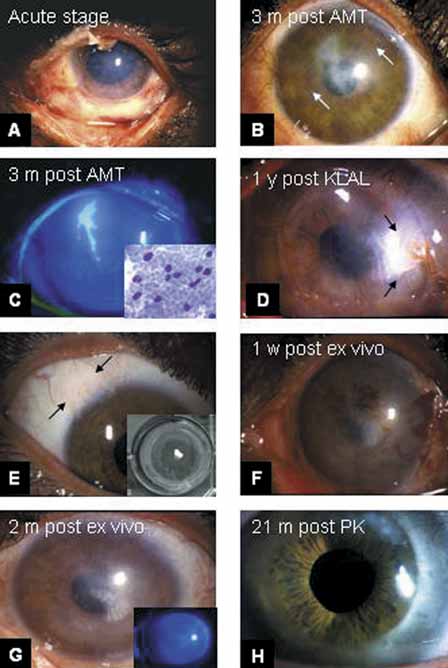
Fig. 14 Ex vivo
expansion. A. In the acute stage, the left eye presented a total
corneal and conjunctival epithelial defect except the temporal bulbar conjunctiva,
stromal edema, and limbal ischemia. B. Three months after AMT as
a patch resulted in total healing with superficial corneal vascularization
(see arrows). C. Recurrent epithelial breakdown occurred because
of total limbal stem cell deficiency (LSCD), which was diagnosed by the
presence of conjunctival goblet cells (i.e., conjunctivalization, of the
cornea [Fig. 14C, inset]) using im-
pression cytology. D. Keratolimbal
allograft transplant (KLAL) was per-
formed 7.5 months after the acute
insult. Nevertheless one segment of the KLAL showed irreversible rejection
with dissolution (see arrows) despite continuous oral cyclosporin. E.
A small biopsy measuring 3 × 2mm was removed from his healthy right
eye (see arrows) and placed on AM fastened to a culture insert. After three
weeks of culturing a confluent layer of approximately 400 mm2 was obtained
(Fig. 14E, inset).
F. One week after transplantation of the composite AM graft with
expanded limbal epithelium, the ocular surface was smooth and intact, with
some blood trapped underneath. G. Two months later the ocular surface
remained quite and smooth without any epithelial defect (Fig.
14G, inset), and the corneal transparency had markedly improved.
H: The corneal epithelium remained intact without conjunctivalization
or epithelial breakdown 21 months after a penetrating keratoplasty. (Modified
from Grueterich M, Espana EM, Touhami A, et al: Phenotypic study of a case
with successful transplantation of ex vivo expanded human limbal epithelium
for unilateral total limbal stem cell deficiency. Ophthalmology 109:1547,
2002, with permission.) |