
|
|
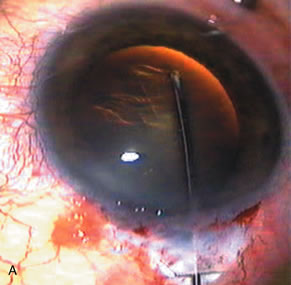
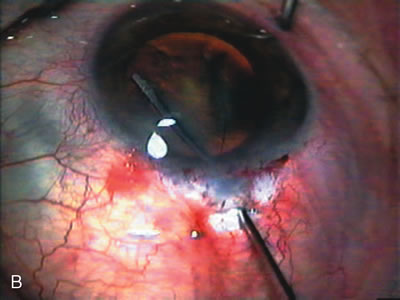
| Fig. 15. Continuous curvilinear capsulorrhexis (CCC), hydrodissection, and paracentesis. A. After achieving adequate pupillary dilation, continuous curvilinear capsulorrhexis (CCC) is most commonly performed with either a bent cystotome and Utrata forceps, or sometimes a combination of both. If the anterior chamber starts to shallow during this maneuver, the surgeon should pause and insert more viscoelastic to prevent the capsular tear from extending into the periphery. CCC is most difficult in patients with very dense nuclei and minimal red reflex, or with miosis. B. After CCC, the surgeon gently lifts the anterior capsule with a 27-gauge cannula and simultaneously directs fluid between the posterior capsule and cortex. Repeat this hydrodissection maneuver in all quadrants to separate cortex from the posterior capsule. Depress the anterior surface of the lens with the shaft of the cannula so that the nucleus does not move too far anteriorly. This practice ensures that the fluid injected separates the cortex from the anterior capsule. C. A paracentesis is essential in order to have a portal for a two-handed nuclear disassembly and lastly to inject balanced salt solution to gauge flow through the scleral flap. |