|
|
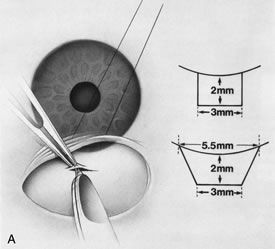
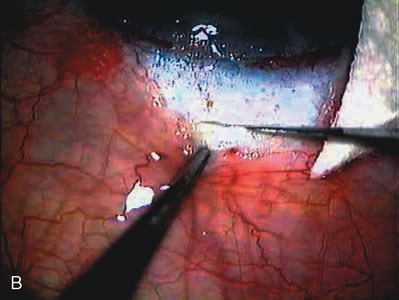
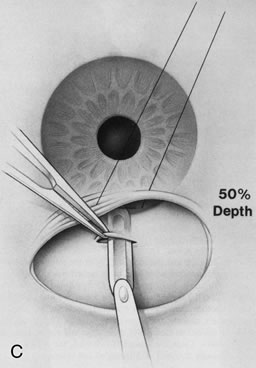
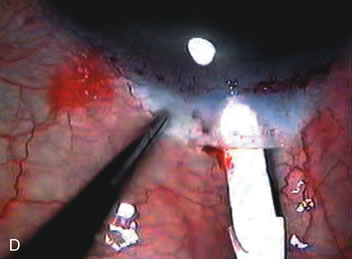
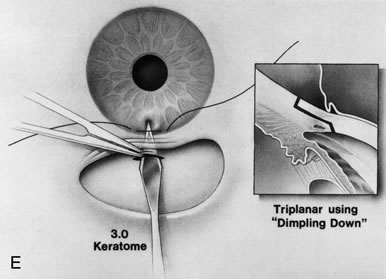
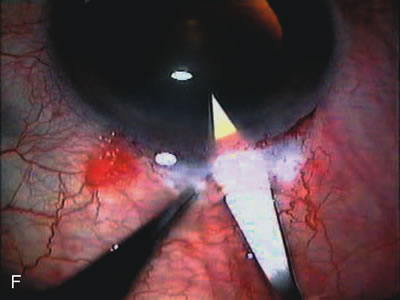
| Fig. 13. Formation of the scleral tunnel. A. and B Use a razor blade or super sharp to start the scleral tunnel 2 to 3 mm posterior to the limbus with a length of 3 mm. The initial depth should be 50% to 75% scleral thickness to achieve the proper plane for tunneling. The sides of the flap are not fashioned at this point until the decision is made on the type of IOL. C and D. Create the scleral tunnel with a crescent blade. The plane of the incision should be kept constant to ensure proper entry through the limbus into clear cornea. The crescent blade should be barely visible through the scleral flap as the surgeon advances the blade 1 mm into clear cornea. As the limbus is approached, reflect the conjunctiva posteriorly if limbus-based, allowing adequate viewing for advancement of the crescent blade into clear cornea. After the angled crescent blade is advanced 1 mm into clear cornea, it is removed. E. and F. A 3-mm keratome follows the same plane of the scleral tunnel to its end, where a dimpling-down of the corneal tissues, followed by anterior chamber entry, ensures a corneal valve effect and triplanar incision. Immediately after removal of the keratome, instill epinephrine underneath the iris to enhance pupillary dilation if necessary. Inject viscoelastic to maintain anterior chamber depth. |