
|
|
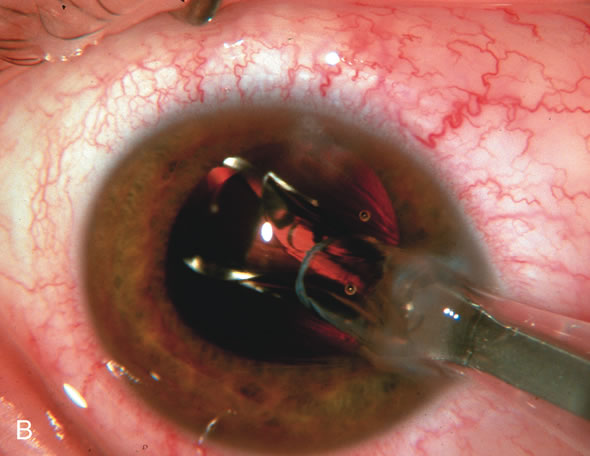
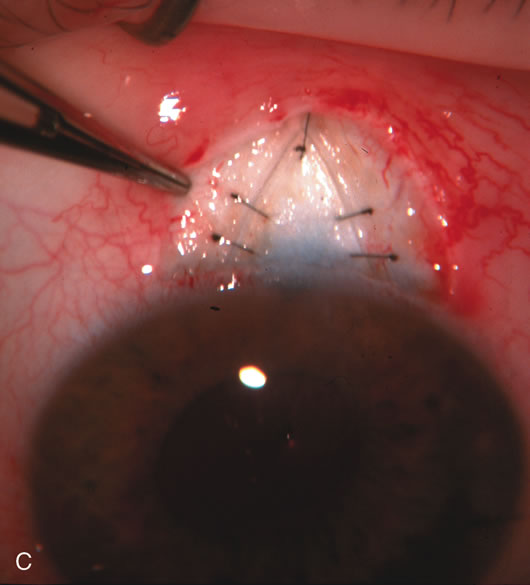
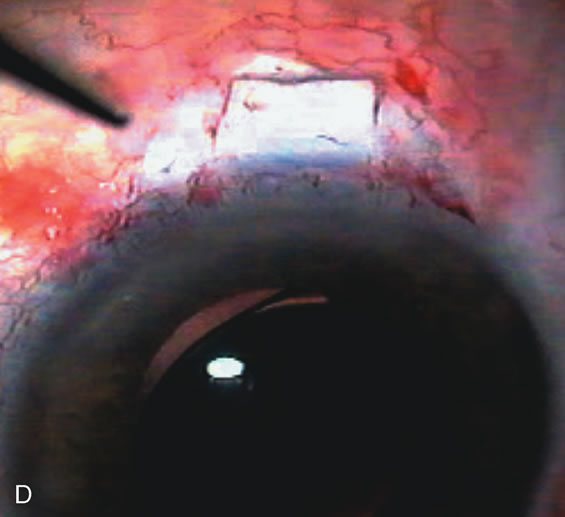
| Fig. 1. The anatomic advantage of small incision cataract surgery for the glaucoma patient. A. Long-term bleb function with a large cataract incision is difficult to achieve with either ECCE-trabeculectomy or trabeculectomy followed later by ECCE. This bleb failed to form sufficiently when combined with large incision ECCE. The inflammation, bleeding, and long-term wound healing with stimulation of fibroblasts associated with this technique are more likely to cause bleb failure. In addition, the increased iris manipulation necessary to deliver the nucleus and subsequent iris repair adds to the long-term breakdown of the blood aqueous barrier. B and C. Two-site phacotrabeculectomy has the advantage of small incision cataract surgery combined with separate site trabeculectomy. The incision size is one third the size of the standard ECCE. The inflammation is less severe, and cataract wound healing is confined to the temporal area. Visual rehabilitation with phacoemulsification and foldable IOL is much faster. Phacoemulsification allows successful lens extraction even in the unfriendly environment of a smaller pupil compared with ECCE. The trabeculectomy is performed in an entirely different site, well away from the wound healing associated with temporal phacoemulsification. The likelihood of this filter functioning long-term is greater than with ECCE-trabeculectomy. D. The surgeon also has the option of single-site phacotrabeculectomy with foldable IOL. Both the lens extraction and trabeculectomy are performed through one small 3.5-mm limbal incision. |