|
|
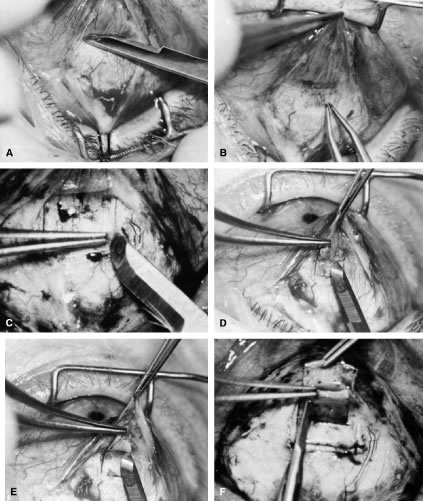
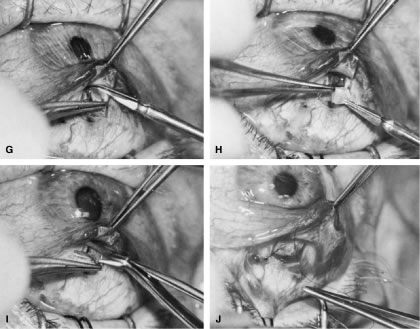
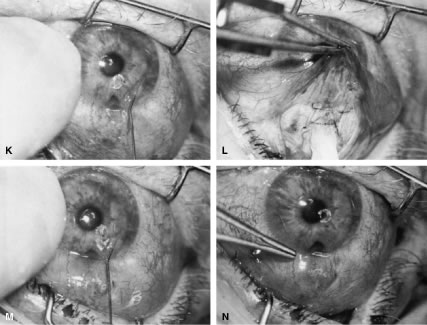
| Fig. 15. Trabeculectomy. A. Episcleral tissue should be cleaned as far anteriorly as the corneoscleral sulcus. B. The sclera is cauterized lightly in the shape of the flap that is to be developed. No cautery is placed on the flap itself, although all bleeding vessels elsewhere on the sclera are coagulated. C. The edge of the scleral flap is held firmly, and a flap is developed with a no. 67 Beaver blade. D. Magnification of at least 10 × with the microscope is preferable when fastening the scleral flap. The blade should be parallel to the bed of the flap. E. Dissection is carried about 2 mm anterior to the junction between the sclera and cornea. F. The radial incision should be carried into clear cornea. G. The block of scleral wall is amputated with Vannas scissors. The tips are inserted under direct visualization. H. The specimen should be inspected to determine whether the posterior trabecular meshwork has been included; it should be given immediately to the nurse for placement in a fixative that will permit pathologic examination. I. Iridectomy of the desired size is performed. J. At least two throws are placed on the first tie to allow the tightness of this suture to be adjusted accurately. K. The anterior chamber is filled with balanced salt solution. The intraocular pressure is monitored carefully with the tip of the finger. L. Additional nonpenetrating sutures near the limbus often are required when the surgeon is trying to avoid gross filtration. M. When filtration is desired postoperatively, a satisfactory bleb should be present at the close of the procedure. N. Normal intraocular pressure has been restored, and a filtering bleb is readily visible. (Spaeth GL. Glaucoma surgery. In Spaeth GL (ed). Ophthalmic Surgery: Principles and Practice. Philadelphia: WB Saunders, 1990.) |