|
|
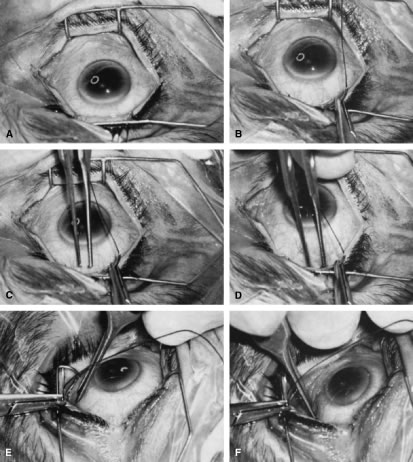
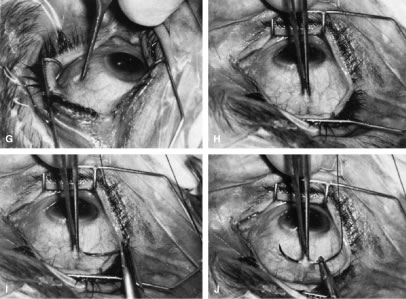
| Fig. 14. Placement of a superior rectus muscle bridle suture. A. The eye with a Barraquer-Colibri speculum in place. The superior rectus muscle is well hidden by the upper lid (lower portion of photograph). B. The needle of a single-armed 4-0 black silk suture is used to retract the upper lid, allowing better visualization of the area in which the superior rectus suture is to be placed. C. The tips of a Lister forceps are held tangential to the superior portion of the globe, approximately 2 mm apart. D. The forceps are moved superiorly so that the tips extend past the insertion of the superior rectus muscle, about 12 mm superior to the lumbus. E. Side view showing the lid held superiorly by the needle of the 4-0 black silk suture and the Lister forceps in its initial position. F. The handle of the forceps is rotated superiorly while the tips are pressed firmly against the globe. The indentation of the globe is caused by the pressure of the forceps. When the forceps have been rotated to the position shown, the tips are closed around the superior rectus muscle. G. After the muscle has been grasped firmly, the forceps are again rotated inferiorly and the globe is pulled inferiorly. H. Surgeon's view of the proper grasp of the superior rectus muscle. I. The needle of the 4-0 black silk suture is placed under the superior rectus muscle not through its belly. J. Proper position of the needle, deep to the forceps and between the globe and the superior rectus muscle belly. (Spaeth GL. Glaucoma surgery. In Spaeth GL (ed). Ophthalmic Surgery: Principles and Practice. Philadelphia: WB Saunders, 1990.) |