|
|
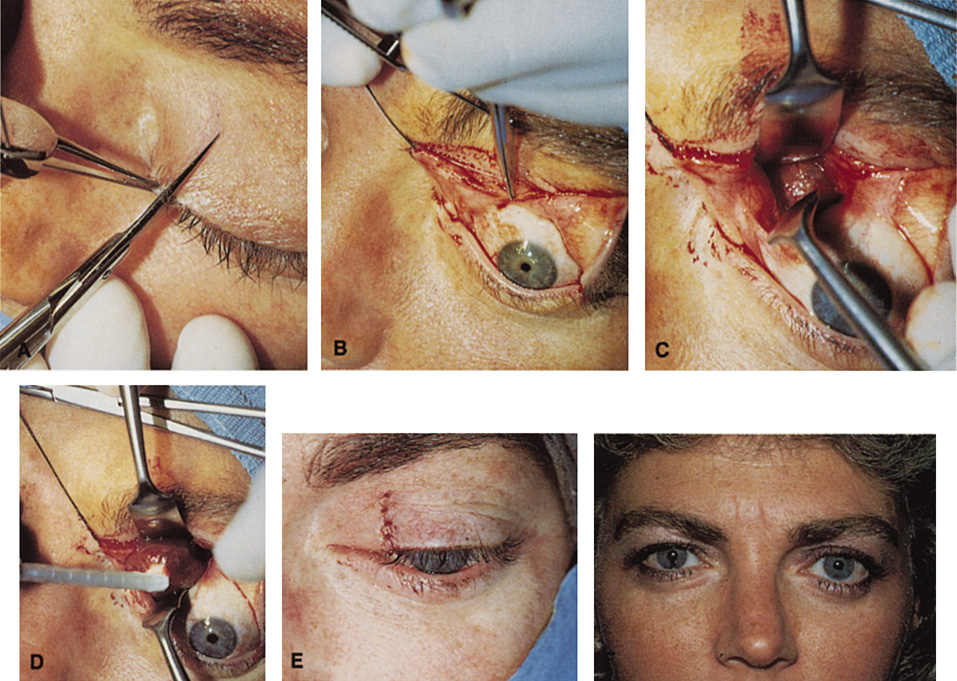
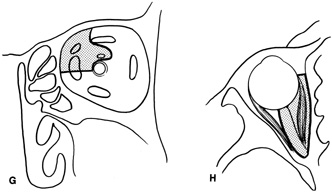
| Fig. 26. A. Straight iris scissors are used to make a full-thickness vertical incision at the junction of the medial and central one-third of the left upper lid. B. The incision is carried through fornix conjunctiva and then can be reflected inferiorly through bulbar conjunctiva as necessary. C,D. Sewall retractors retract the superior oblique muscle above and the globe laterally, so that dissection can be carried to the peripheral and intraconal spaces where the lesion is identified and removed with the aid of a cryoprobe (D). E. Full-thickness lid incision is reapproximated. F. Postoperative appearance of the patient. Excellent scar camouflage is afforded by the vertical incision placed within the eyelid skin. Schematic of areas of orbit amenable to the vertical-lid split anterior approach. Coronal (G) and axial (H) views. |