|
|
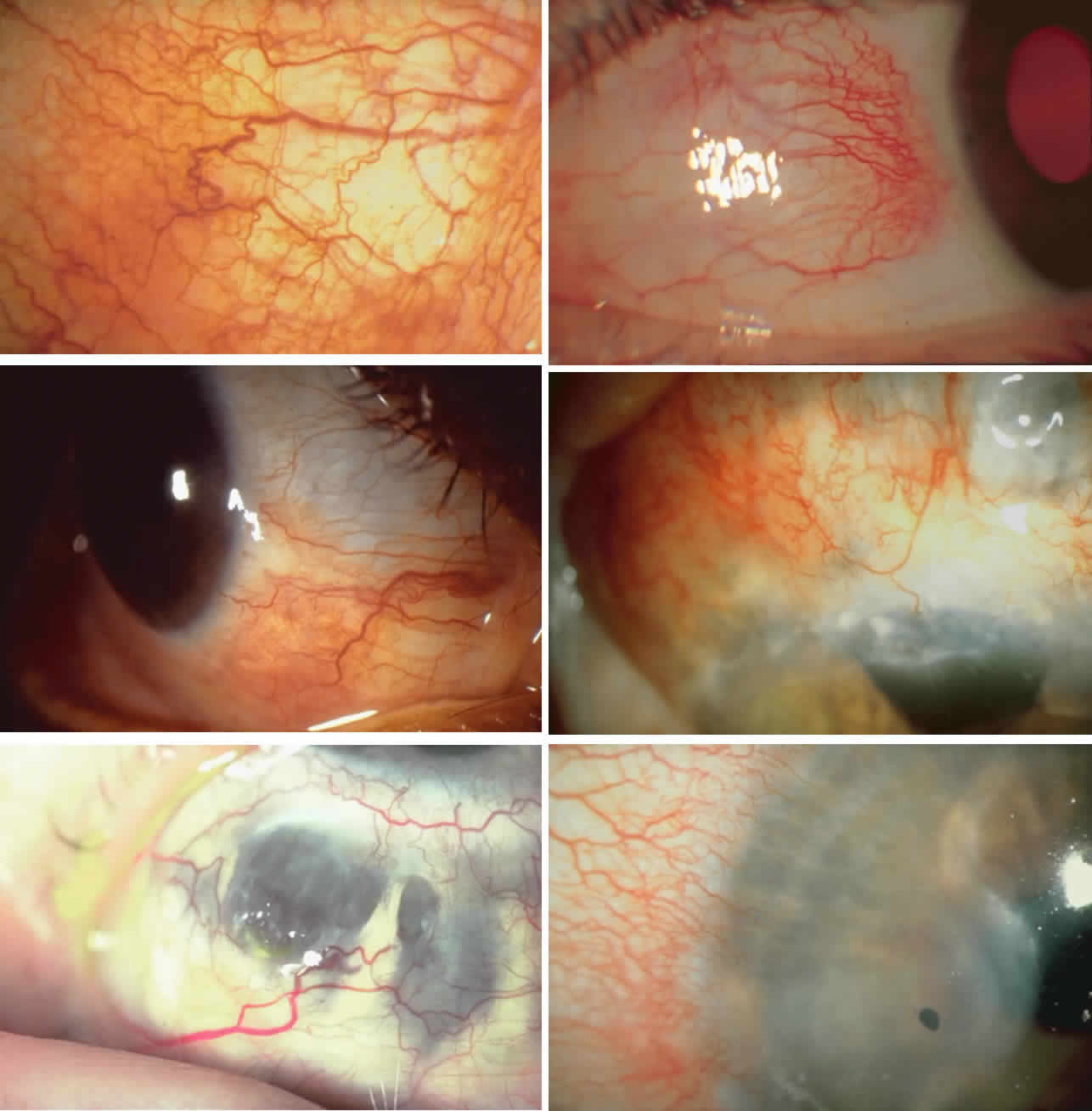
| Plate 1. A. Simple episcleritis. There is a diffuse dilatation of all the vessels, but the normal vascular pattern is not disturbed. The episcleral tissue is edematous but there is no swelling of the sclera. B. Nodular episcleritis. The episclera is edematous in the area of the nodule. The vessels over the nodule are dilated, but there is no displacement of the deep vessels, so the sclera is not edematous. C. Diffuse scleritis. The sclera is inflamed and swollen below the horizontal meridian, and the vessels are irregular and distorted. Above the horizontal, where there was previously inflammation, the color of the sclera has changed. This is not due to thinning of the sclera but rather to an increased transparency as a consequence of the alteration of the proteoglycan/collagen structure caused by recurrent inflammation. D. Sclerokeratitis in diffuse scleritis. Diffuse scleritis recurring at the same site often leads to opacification of the corner adjacent to it. This is caused by transudate from leaking vessels and sometimes leads to an immune ring in the cornea at this site. E. Necrotizing scleritis in Wegener's granulomatosis. There is an intense inflammatory response with granulomatous changes and necrosis of the sclera. The vessels are grossly distorted and the inflammation transgresses the limbus. The vessels that are entering the cornea leak profusely, and there is early erosion of the peripheral corneal tissue. F. Scleromalacia perforans. Quiet sequestration of the sclera in a 52-year-old woman with long-standing burned-out erosive articular rheumatoid arthritis. Note the complete lack of an inflammatory response even though this is at an active stage of the resorption of the tissue. |