|
|
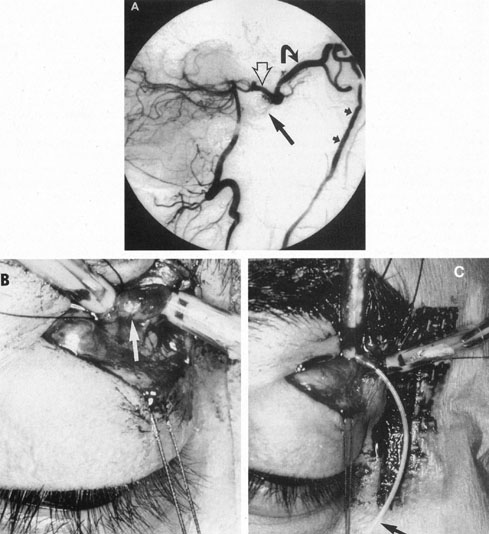
| Fig. 21. A 35-year-old man with a right carotid cavernous fistula (CCF) following head trauma. Therapeutic alternatives in this case were limited by the presence of an occlusive dissection of the ipsilateral right internal carotid artery and absence of venous access to the fistula via the inferior petrosal sinus. The lesion was embolized initially via the ipsilateral posterior communicating artery (arrow in A indicates coils from the first procedure). However, the fistula recanalized, and the patient presented with recurrent symptoms. A: Lateral projection of the left vertebral artery at the start of the second procedure demonstrates opacification of the supraclinoid right internal carotid artery (open arrow), with fistulous flow to the superior ophthalmic vein (curved arrow), draining inferiorly via the facial veins (small arrows). The second procedure was performed with surgical exposure of the superior ophthalmic vein under general anesthesia in the angiography suite. B: The tense distended vein (white arrow) has been dissected and secured with two vascular ties. C: A small venotomy was performed between the vascular ties through which a Tracker 18 microcatheter (small arrow) was inserted. This was then guided over a wire into the cavernous sinus in the region of the fistula, where a further packing of coils resulted in complete occlusion of the CCF. (Courtesy of Dr. Peter Rubin.) |