|
|
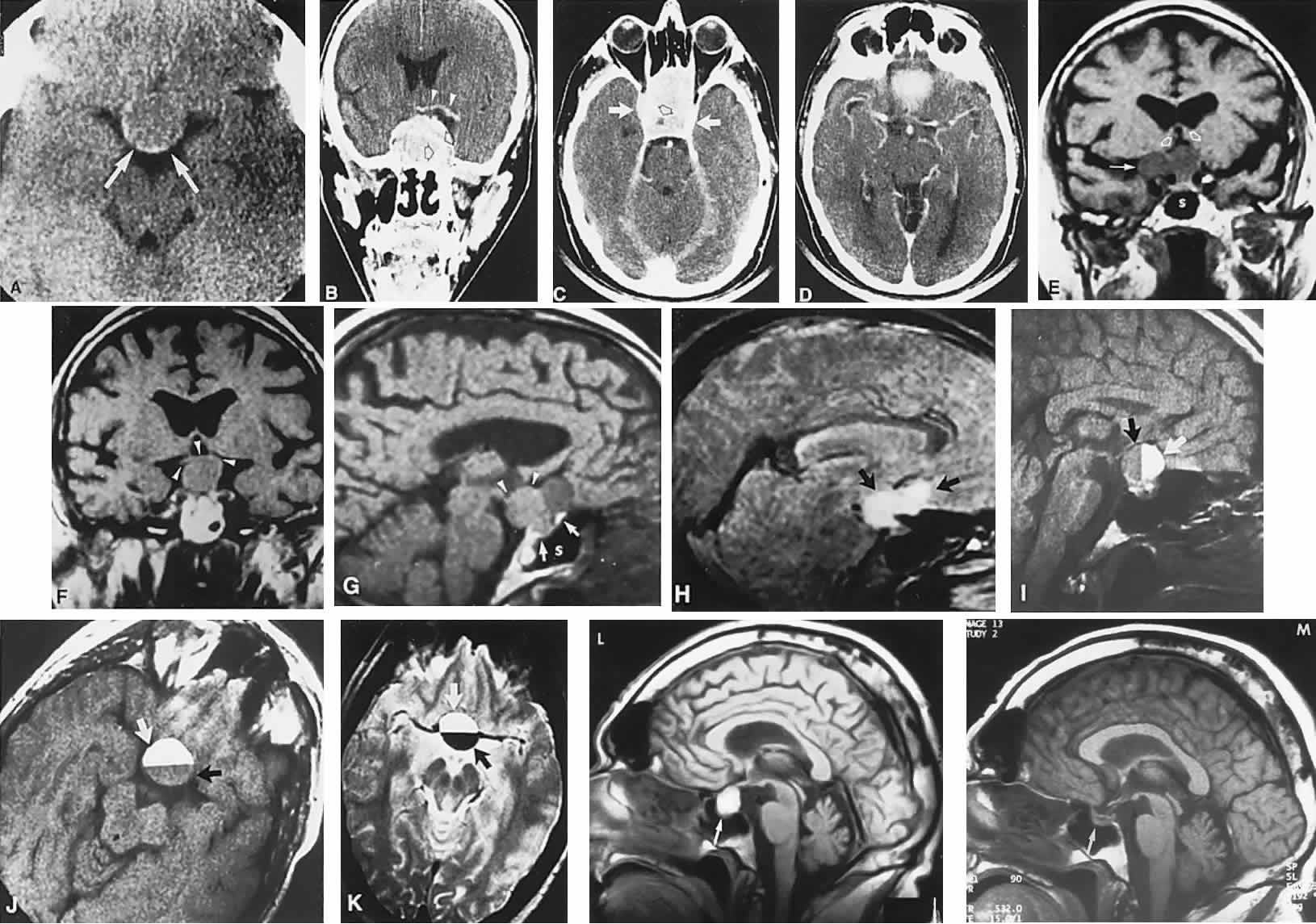
| Fig. 3. Neuroimaging of pituitary adenomas. A. Axial computed tomography (CT) section shows a round tumor mass filling the suprasellar cistern; ring enhancement (arrows) indicates subcapsular hemorrhage. B. Contrast-enhanced coronal CT section through a large invasive adenoma. Note encasement of the carotid artery (arrows) and the position of the middle cerebral artery above (arrowheads). C. Axial CT section shows lateral expansion into the cavernous sinuses (white arrows) and a necrotic cyst (black arrow). D. Subfrontal superior extent of the mass. Note the middle cerebral arteries. E. Magnetic resonance imaging of a large lobulated prolactinoma, with suprasellar extension. Note the distortion of the third ventricle (open arrows) and extension toward the temporal lobe (long arrow); the tumor has not involved the sphenoidal sinus (s). F. Chiasm (arrowheads) is draped on the superior surface of the tumor (TR, 550 milliseconds; TE, 26 milliseconds). G. Sagittal section shows suprasellar growth with the chiasm above (arrowheads); the sella (arrows) and sphenoidal sinus (s) are normal (TR, 850 milliseconds; TE, 26 milliseconds). H. Hyperintense signal (TR, 2000 milliseconds; TE, 60 milliseconds) indicates the partial cystic character. Sagittal (I) and axial (J) sections with head tilt to the right, in case of a large cystic adenoma with an interface level between newer blood (white arrow) and older blood (black arrow) (TR, 800 milliseconds; TE, 30 milliseconds). K. Signal difference is intensified (TR, 2100 milliseconds; TE, 80 milliseconds). L. Hemorrhage (bright signal, arrow) in a pituitary adenoma with headache and bitemporal field depressions. M. Without interventions, 2-month follow-up showed spontaneous involution, with normal pituitary gland (arrow), stalk, and chiasm. |